Created 2009.
Cutaneous signs can be a clue to the diagnosis of systemic diseases or may be a complication of them requiring specific attention. More details on specific skin conditions can be found in other parts of the course or On DermNet.





Hypercorticism can result in acne, striae and cutaneous atrophy.


Growth hormone excess results in soft tissue hypertrophy, skin tags and seborrhoea.

Lack of cortisol increases ACTH with resultant generalised hyperpigmentation.



Chronic renal failure is associated with:



Renal transplantation and the use of immunosuppressive medication gives rise to a high risk of viral infections (mainly warts) and skin cancers (especially squamous cell carcinomas). These may be very aggressive.
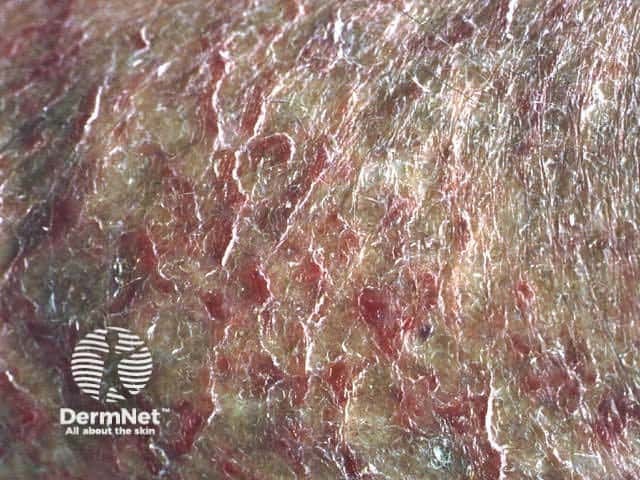
Porphyrias are due to abnormalities of the haem pathway and result in cutaneous photosensitivity. Diagnosis is confirmed by detection of excessive porphyrins in blood, urine or faeces. The most common to present to dermatologists are:







Vitamin C deficiency presents with corkscrew hairs and bleeding gums or easy bruising and may occur in the elderly. Low levels of leucocyte ascorbic acid confirm the diagnosis.
Nicotinic acid deficiency presents with photosensitive eruption on neck and feet, diarrhoea and dementia.
Protein deficiency may cause dry red skin and hair and is associated with oedema and ascites.
Fatty acid deficiency in infants or with total parenteral nutrition may result in dry red skin and delayed healing.





Sarcoidosis is diagnosed histologically by the presence of noncaseating granulomas in the skin, lymph nodes, lungs, liver, spleen, eyes, parotid glands or joints. The mainstay of treatment is systemic corticosteroids.
Cutaneous features are highly variable:






Acquired immunodeficiency syndrome (AIDS) is due to infection of T cells with human immunodeficiency virus (HIV) resulting in progressive immunodeficiency and a decrease in T-cell helper / suppressor ratio.
A variety of cutaneous inflammatory conditions, infections and malignancies arise and tend to be more vigorously expressed than in normal individuals.
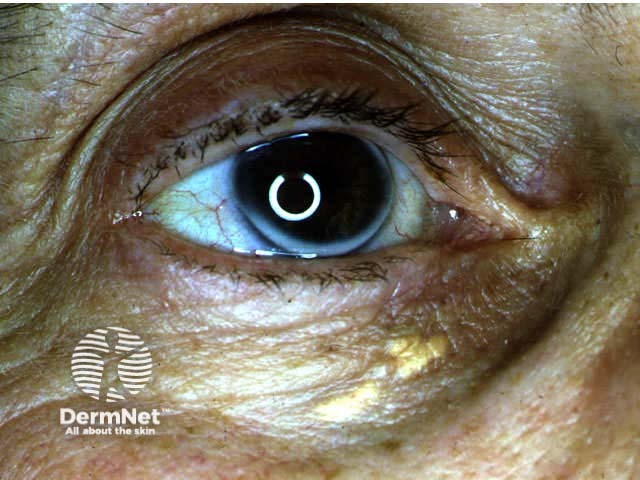
How may xanthelasma be removed?
Information for patients

