What is chromoblastomycosis?
Chromoblastomycosis is a chronic fungal infection in which there are raised crusted lesions affecting the skin and subcutaneous tissue. It usually affects the limbs.
Chromoblastomycosis


What causes chromoblastomycosis?
Chromoblastomycosis may be due to several fungi found in soil, wood and decaying plant material.
The organism is inoculated into the skin by a minor injury, for example, a cut with a splinter when barefoot. It is exceedingly rare in New Zealand, but relatively common in warmer areas such as the Pacific Islands.
The most common organisms are:
- Phialophora verrucosa
- Fonsecaea pedrosi
- Fonsecaea compacta
- Cladophialophora carrionii
- Rhinocladiella aquaspersa (Ramichloridium cerophilum).
What are the clinical features of chromoblastomycosis?
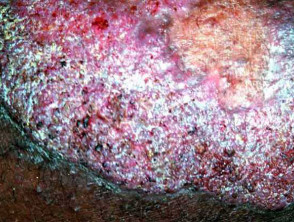
Chromoblastomycosis generally presents as a single lesion on an exposed site such as the foot or hand.
- It starts as a small firm red or grey bump.
- It grows very slowly: only about 2mm per year.
- Eventually, a warty dry nodule or plaque develops.
- There may be at least partial clearing with scarring in the centre of the lesion.
- The affected limb can enlarge generally (elephantiasis).
- New lesions may develop in time as satellites around the first one or the infection may be scratched into a new site.
- It may cause no discomfort but is frequently very itchy.
- Rarely, squamous cell carcinoma (SCC) develops within longstanding chromoblastomycosis.
The infection is sometimes confused with other skin conditions such as:
- Other fungal infections such as sporotrichosis
- Bacterial infections such as atypical mycobacterium infection, tuberculosis, leprosy and syphilis
- Protozoal infections such as leishmaniasis
- Squamous cell carcinoma
- Skin disorders such as psoriasis, discoid lupus erythematosus.
Chromoblastomycosis



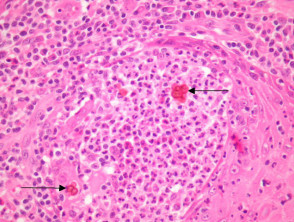
How is chromoblastomycosis diagnosed?
Histopathology of chromoblastomycosis may show typical thick-walled dark-brown 'sclerotic' cells on skin biopsy confirming the presence of a dematiaceous fungus. It is dark coloured due to melanin in the walls of the organism.
Culture in Sabouraud medium with antibiotics at 25–30 degrees celsius grows olive-green to black fungal colonies after one or two weeks. Naming the responsible fungus can be difficult. Phaeohyphomycosis is the name given to an infection caused by dematiaceous fungi.

What is the treatment for chromoblastomycosis?
Rarely, chromoblastomycosis resolves spontaneously leaving a scar.
Treatment is difficult and prolonged. It may include:
- Itraconazole, posaconazole or voriconazole, possibly in combination with terbinafine
- Flucytosine
- Thiabendazole
- Local heat
- Cryotherapy
- Surgery to remove the affected tissue completely.