Introduction
There are several distinct clinical forms of angiofibroma which share identical histopathology:
- Fibrous papule
- Pearly penile papules
- Angiofibroma associated with tuberous sclerosis
- Syndromal angiofibroma.
Histology of angiofibroma
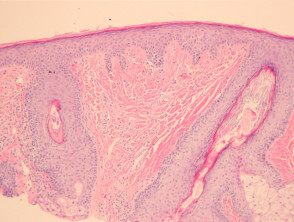
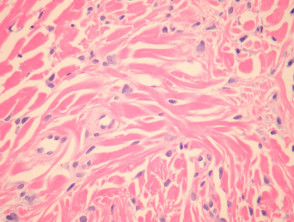
Angiofibromas cause a dome-shaped mass in the superficial dermis (figure 1). The overlying epidermis is uninvolved but may be atrophic. The lesion is characterized by a proliferation of stellate and spindled cells around blood vessels (figure 2). There are coarse concentric collagen bundles (figures 1, 2). Comparing the density of the collagen of the lesion with the surrounding dermis, which should be looser or elastotically damaged, can be a helpful diagnostic clue. Occasionally, a sparse inflammatory cell infiltrate of lymphocytes is present.
Several histological subtypes have been described:
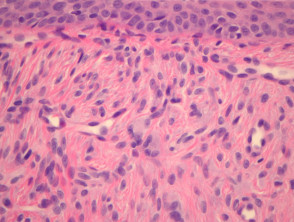
- Hypercellular angiofibroma is characterised by an increased number of stellate and spindled cells (figure 3).
- Clear cell angiofibroma shows a proliferation of granular to foamy cells, resembling histiocytes.
- Pleomorphic angiofibroma is characterized by bizarre, stellate fibroblasts.
- An epithelioid variant of angiofibroma consists of epithelioid-type cells with pink cytoplasm and prominent nucleoli.
Angiofibroma pathology
Special studies for angiofibroma
Dermal dendritic cells usually stain for factor XIIIa. S100 is negative.
Differential diagnosis of angiofibroma pathology
Sclerosing naevus — These usually do not exhibit vascular ectasia. S100 stain will highlight the melanocytes, and will be negative in fibrous papules.
Capillary haemangioma — These lack the fibrous stroma with stellate fibroblasts and dense collagen.