Neurofibromas are common tumours that may occur either as a solitary lesion or in multiplicity (neurofibromatosis).
Histology of neurofibroma
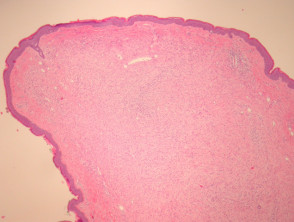
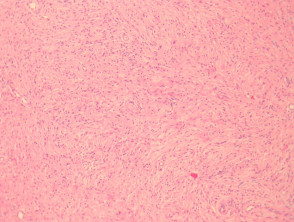
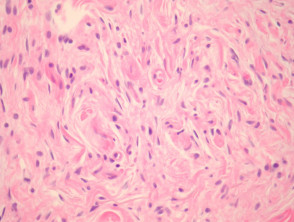
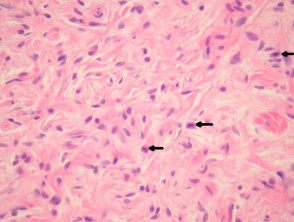
In a neurofibroma, sections show a non-encapsulated lesion in the dermis (figure 1). These lesions represent a proliferation of all elements of peripheral nerves. The cells have wavy serpentine nuclei and pointed ends (figures 2-4). There is stromal mucin deposition and fibroplasia (figures 2-4). Mast cells are usually easy to find (figure 4, arrow). Axons course through the tumour and though difficult to see on routine sections may be illustrated with immunohistochemical stains for neurofilament.
Plexiform neurofibroma is a subtype in which the tumour grows within and irregularly expands a nerve bundle. Though large plexiform neurofibromas are thought to be diagnostic of NF1, a plexiform pattern may be seen in solitary skin lesions that are of little clinical significance.
Neurofibroma pathology
Special studies for neurofibroma
Positive stains: S100, CD34+ (focal)
Negative stains: EMA (except in plexiform neurofibromas in which EMA stains the surrounding perineurium of the nerve bundle).
Differential diagnosis of neurofibroma pathology
Schwannoma – Shows Antoni A and B pattern and is encapsulated. Plexiform neurofibroma may resemble schwannoma. Neurofibromas typically have axons coursing through the mass, which stain with neurofilament immunohistochemically.
Perineurioma – These are EMA positive and S100 negative.
Dermatofibromasarcoma protuberans – These are positive with CD34, and lack S100 positivity.