Introduction
Primary cicatricial alopecias comprise a group of disorders in which there is permanent destruction of the hair follicle. This results from irreversible injury of the stem-cell-rich bulge area, which is required for the cyclic regeneration of the lower portion of the hair follicle. Histopathological examination helps in identifying the underlying disorder through the type of infiltrate surrounding the follicles, together with other pathological characteristic features.
Neutrophilic cicatricial alopecia
Folliculitis decalvans (FD)
Introduction and clinical picture
Folliculitis decalvans is a primary cicatricial alopecia with neutrophilic infiltrate predominance.
FD manifests as recurrent follicular pustules that affect mainly the vertex and occipital area of the scalp of middle-aged males. Other clinical findings include erythema, dark yellow-gray scales, follicular hyperkeratosis, erosions, and hemorrhagic crusts, most prominent around the follicles. In advanced stages, atrophic patches with hair tufting are observed.
Trichoscopic features
Characteristic signs:
- Tufts of 5–20 or more upright hairs emerging from a single dilated orifice (polytrichia) surrounded by yellowish scales
- Doll’s hairs.
The above-mentioned signs are the most sensitive and specific dermoscopic findings of folliculitis decalvans.
- Whitish areas representing fibrosis around follicles (starburst sign)
- Follicular pustules
- Yellowish discharge and crusting.
Other features:
- White and milky red areas with no follicular ostia representing cicatrization in late-stage disease
- Concentric vessels of no characteristic pattern around hair follicles
- Thickened, interfollicular, keloid-like areas
- Broken hairs
- Vellus hairs
- Keratotic plugs.
Folliculitis decalvans



Dissecting cellulitis
Introduction and clinical picture
Dissecting cellulitis (dissecting folliculitis, perifolliculitis capitis abscedens et suffodiens) is a neutrophilic primary cicatricial alopecia characterised by chronic, progressive inflammation that occurs most commonly in dark-skinned young adults. The primary event is occlusion of follicular openings on the scalp vertex or occiput.
Later in the course of the disease, perifollicular pustules, nodules, and fluctuant abscesses with interconnecting sinus tracts with seropurulent discharge, tufted hairs and keloidal lesions may be present. It is considered one of the follicular occlusion tetrad, including acne conglobata, hidradenitis suppurativa, and pilonidal sinus.
Trichoscopic features
In early stages, features of non-cicatricial alopecia that are found on trichoscopy include:
- Yellow dots that sometimes show a ‘three-dimensional’ structure or ’soap bubble’ appearance surrounding dystrophic hair shafts
- Black dots
- Broken hair
- Exclamation mark hairs
- Circular hairs
- Empty follicular openings
- Peri- and inter-follicular scales
- Erythema
- Yellowish crusts
- Large brown dots
- Polytrichia
- Punctate vessels
- Red dots
- Blue gray dots
- Short regrowing hairs
- Honeycomb pigmentation
- Pili torti.
Late-stage features that appear on trichoscopy include:
- Yellow structureless areas, confluent ivory-white or amorphous white areas with absent follicular openings
- Cutaneous clefts with emerging hairs.
Lymphocytic cicatricial alopecia
Discoid Lupus Erythematosus (DLE)
Introduction and clinical picture
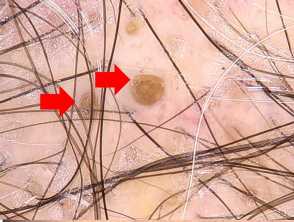
Discoid lupus erythematosus is one of the most common causes of primary cicatricial alopecia with lymphocytic infiltrate predominance. DLE is manifested by one or more erythematous atrophic plaques of alopecia with follicular plugging, adherent scales, telangiectasia, hypo- and hyperpigmentation. End stage disease shows fibrotic, atrophic, smooth white plaques with absent follicular openings. Long-standing DLE cannot be distinguished clinically from other diseases in the spectrum of primary cicatricial alopecia.
Trichoscopic features
Active DLE:
- Yellow dots are markedly large due to follicular plugging
- Thick arborizing vessels
- Speckled brown pigmentation and blue-gray dots corresponding to melanin incontinence on histopathology
- Peripilar white halo
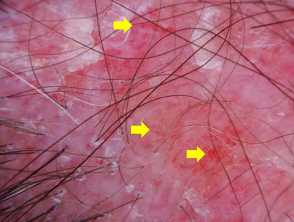
- Follicular red dots which is considered a good prognostic factor for hair regrowth.
Discoid lupus erythematosus

Late stage DLE:
- Large yellow dots
- Lack of follicular openings.
- Structureless milky red or white areas denting fibrosis.
- Arborizing vessels also may be present.
- Significant increase of shiny white structures i.e. crystalline and rosettes may be observed.
Discoid lupus erythematosus

Classic Lichen Planopilaris (LPP) and Graham Little Syndrome
Lichen planopilaris includes three main subgroups; Classic LPP, Graham Little syndrome, and frontal fibrosing alopecia.
Introduction and clinical picture
Patients with classic LPP are typically around the age of 50, and women are more often affected than men. Patients may complain of itching, burning, and scalp sensitivity. LPP is characterised by irregular atrophic patches with follicular hyperkeratosis and perifollicular erythema. The scalp in Graham Little syndrome shows lesions of classic LPP, while axillary and pubic areas show non-scarring alopecia; there is also keratosis pilaris on the trunk and extremities. Alopecia of the eyebrows may be found in some cases.
Trichoscopic features of classic lichen planopilaris
Trichoscopic features vary according to stage of the disease and the degree of activity.
Active stage:
- Perifollicular hyperkeratosis
- Peritubular casts
- Elongated linear blood vessels
- Violaceous areas
- Blue grey dots
- Follicular and perifollicular erythema.
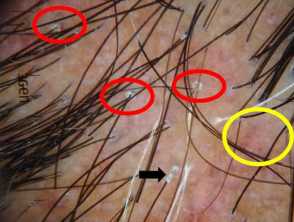
Irregularly distributed follicular openings (red arrows) denoting scarring (cicatricial) alopecia Perifollicular scales (red circles, peritubular cast (black arrows) and blue grey dots (yellow circles) in lichen planopilaris Scaly scalp showing perifollicular scales in a female patient with lichen planopilarisLichen planopilaris

Inactive and late-stage:
- White dots are large and irregular
- Loss of follicular ostia
- White fibrotic and milky red areas
- Tufted hairs
- Broken hairs.
Trichoscopic features of Graham Little syndrome
Scalp lesions
- The same features seen in classic LPP.
Axillae and pubic lesions
- Yellow dots.
Lichen planopilaris

Frontal Fibrosing Alopecia
Introduction and clinical picture
Frontal fibrosing alopecia is a primary lymphocytic cicatricial alopecia within the spectrum of lichen planopilaris; affecting mainly postmenopausal women. Frontal fibrosing alopecia is characterised by band-like alopecia affecting the frontal hairline. Follicular hyperkeratosis and perifollicular erythema can often be found in the first hairs of the hairline. Alopecia of the eyebrows is a frequent finding.
Trichoscopic features
Scalp lesions:
- Absent follicular openings
- Follicular hyperkeratosis
- Perifollicular erythema may be considered a sign of disease activity
- Follicular openings with only one hair predominating in the hair-bearing margin
- Lonely hairs may be observed
- Absence of vellus hair
- Ivory white background in the early fibrotic stage.
Eyebrow lesions:
- Dystrophic hairs
- White areas
- Eyebrow regrowth in distinct directions reflecting the fibrosing process.
The above three features are considered characteristic signs.
- Regularly distributed red or gray dots throughout the course of the disease
- Loss of follicular openings in advanced disease.
Pseudopelade of Brocq
Introduction and clinical picture
Pseudopelade of Brocq is a primary cicatricial alopecia with lymphocytic infiltrate predominance. Classic pseudopelade of Brocq affects mostly women between the ages of 30 and 50 years. It usually presents with small flesh-colored alopecic patches with irregular margins, a pattern described as “footprints in the snow.”
Unlike DLE and LPP, follicular hyperkeratosis and perifollicular or diffuse erythema are mostly absent. There is a possible clinical overlap in presenting features between DLE and LPP. Clinically and dermoscopically, pseudopelade of Brocq is a diagnosis of exclusion as non-specific features are usually seen.
Main trichoscopic features:
- Reduced number of follicular ostia.
- White, porcelain, gray, beige, erythematous and milky white areas.
- Interfollicular areas show prominent honeycomb pigment pattern in dark skin phototypes (IV and V) and pinkish-white areas in light skin phototypes (I, II and III) are observed.
- Occasionally solitary dystrophic hairs at the periphery of the lesion.
- Characteristic trichoscopic features of other primary cicatricial alopecias are absent.
Central centrifugal cicatricial alopecias (CCCA)
Introduction and clinical picture
Many factors are incorporated in the pathogenesis of CCCA including genetic factors and hair styling practices. CCCA affects females of African descent. It is characterized by slowly progressive thinning of hair on the vertex with follicular pustules, tenderness, and sometimes pruritus.
Trichoscopic features
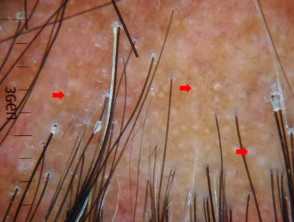
- Peripilar whitish halo corresponding histopathologically to lamellar fibrosis surrounding the outer root sheath is considered the most sensitive and specific trichoscopic finding of early and late stage CCCA.
- Asterisk-like brown blotches, broken hairs and dark peripilar halos are considered particular features of CCCA.
- Pinpoint white dots irregularly distributed.
- White patches.
- Honeycomb pigmentation.
- Erythema.
- Scaling.
Mixed infiltrate alopecia
Erosive pustular dermatitis of scalp
Introduction and clinical picture
Erosive pustular dermatosis commonly affects older individuals. It is characterized by a pustular eruption, erosions, and crusting that heal with scarring.
Trichoscopic features using high magnification
Active phase:
- Perifollicular serous, black-yellow crusts
- Patchy brown-gray skin hyperpigmentation
- Tortuous and curved hair shaft like pili torti
- Broken hair shafts a few millimeters above the scalp level
- Hair tufting with no more than 4 hairs emerging from the same unit.
Chronic phase:
- Marked atrophic scalp with visible anagen bulbs
- Absent follicular openings
- Prominent telangiectasia with milky red and white areas
- Follicular yellow thick exudate.