What is ultraviolet radiation?
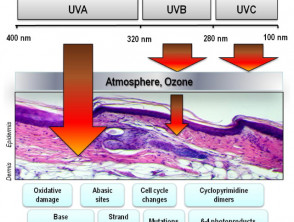
Ultraviolet radiation (UVR) forms part of the electromagnetic spectrum — the energy emitted from the sun. UVR is categorised according to wavelength, which ranges from 100–400 nm.
- UVR is involved in tanning, accelerated skin ageing, ocular damage, and the development of skin cancer.
- UVR also has beneficial effects due to the production of vitamin D in the skin and its immune-modulating effects on inflammatory skin diseases.
Other sources of ultraviolet radiation
Artificial sources of UV include tanning booths and mercury vapour lighting; some halogen, fluorescent, and incandescent lights; and some forms of lasers.
Types of ultraviolet radiation
Ultraviolet A radiation
- Ultraviolet A radiation (UVA) is long wavelength UVR (wavelength: 315–400 nm).
- UVA passes through the whole atmosphere and accounts for 95% of UVR reaching the Earth's surface.
- It penetrates through an individual's epidermis into the dermis.
- UVA has lower energy than ultraviolet B radiation (UVB) and causes less damage per photon.
- It contributes to sunburn, ageing skin, and skin cancer through oxidative injury (cell damage from free radicals).
- UVA stimulates epidermal melanin oxidisation (immediate tanning) and melanin production (delayed tanning), which protect the skin by absorbing UVR within the epidermis.
Ultraviolet B radiation
- UV-B is medium wavelength UVR (wavelength: 280–315 nm).
- Most solar UVB is filtered by the atmosphere.
- It penetrates into an individual's epidermis but not into their dermis.
- UV-B has high energy and damages epidermal cell DNA.
- It stimulates melanin production.
- UV-B is the main cause of sunburn and some forms of skin cancer.
Ultraviolet C radiation
- Ultraviolet C radiation (UVC) is short-wavelength UVR (wavelength: < 280 nm).
- Solar UV-C is completely absorbed by the atmosphere and doesn’t reach the Earth’s surface.
- UV-C can be emitted by artificial sources of UVR (eg, by welding arcs and mercury vapour lamps).
- Although shorter UVR wavelengths do not penetrate through the skin, UV-C has higher energy than UVB and injures the skin surface.
- Exposure to UV-C can lead to severe but superficial sunburn.
Electromagnetic spectrum of visible and ultraviolet radiation and biological effects on the skin
Ultraviolet Index
The Ultraviolet Index (UVI) is a measure of the strength of UVR causing erythema (sunburn). If the UVI is > 10, the UVR is extreme, and if it is < 3, it is low.
Factors that result in greater exposure to ultraviolet radiation
The UVI is higher and UVR is more intense closer to the equator compared to the UVI and UVR at longer latitudes, as the sun is overhead so the distance to reach the Earth is shorter. UVR levels are also greater:
- During the summer months and during the middle of the day, when the angle of the sun is the smallest
- At higher altitude, when the atmosphere is thinner
- On a clear day, compared to a cloudy day or where the atmosphere is polluted
- Around reflective surfaces, such as snow, sand, grass, or water
- In the Southern Hemisphere compared to the Northern Hemisphere, as there is less separation between the sun and the Earth:
- Relative to the Northern Hemisphere, New Zealand is exposed to 40% higher peak UVI at commensurate latitudes
- If the ozone layer is depleted.
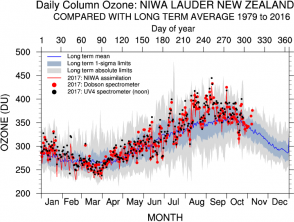
The National Institute of Water and Atmospheric Research (NIWA Taihoro Nukurangi) Lauder ozone measurements taken at Lauder in Central Otago show seasonal and annual climatological variability. Ozone column amounts are measured in Dobson units (DU), where 1 DU = 2.69 x 1016molecules/cm2.
Ozone variation in 2016 in Lauder, New Zealand
What is the ozone layer?
Ozone is a trace gas that forms the ozone layer within the stratosphere, which is part of the atmosphere around the Earth.
- There are three molecules of ozone for every 10 million molecules of air.
- Ozone is a highly reactive molecule that contains three oxygen atoms.
- Ozone absorbs solar UVR, which heats the atmosphere.
- Ozone also shields the Earth from the biologically harmful effects of UVR.
- Reduced ozone leads to higher levels of UVR on the Earth’s surface.
The ozone hole and the Montreal Protocol
- Ozone-depleting substances (ODSs) such as chlorofluorocarbons (CFCs; also known as Freons) and Halons, once used in refrigerators, spray cans, and fire extinguishers, have reduced the amount of ozone in the stratosphere.
- When CFCs reach the upper atmosphere, they are exposed to UVR, which causes them to break down and form chlorine gas. Chlorine reacts with the oxygen atoms in ozone and rips apart the ozone molecule.
- Over 50% of the ozone in the Antarctic stratosphere has been depleted, leading to the formation of the springtime ‘ozone hole’. During summer, ozone-depleted air from the ozone hole can drift over to South America and New Zealand, resulting in higher levels of UVR than usual for the latitude.
- Higher winter UVR levels in Australia were seen in the 1990s compared with the 1970s, resulting in predictions that the incidence of UVR-related skin cancer will rise due to depleted ozone levels.
The ‘Montreal Protocol on Substances that Deplete the Ozone Layer’ was signed in 1987. It is an international environmental agreement to protect the ozone layer by reducing the production and usage of ODSs such as CFCs. Since its initiation, the atmospheric levels of ODSs have significantly decreased and the stratospheric ozone is expected to fully recover by the year 2050.
How does ultraviolet radiation affect the skin?
- UVA induces oxidative damage to the DNA in the presence of melanin.
- UVB causes damage independently of independent of melanin and directly affects DNA.
- The UVB-induced release of pro-inflammatory cytokines causes sunburn, which is maximum about 8 hours after exposure. Peeling is accompanied by cellular apoptosis.
- DNA damage also causes the loss of structural integrity in the skin and photo-ageing.
- The accumulation of unrepaired DNA and UVR induced immunosuppression, increase the risk of mutations and the development of skin cancer.
Protective mechanisms
- Tanning is due to a series of complex steps that are triggered by UVR induced damage to DNA and other components of the skin.
- The thickness of the epidermis is increased in response to growth factors released by injured keratinocytes.
The chronically sun-exposed skin of a bald scalp or face, neck, and hands has unique characteristics compared to skin that has not been exposed to UVR.
- Photo-aged skin is thinner than non-sun-exposed skin in the same individual.
- Photo-aged skin is dryer. Over time, actinic keratoses appear in the most sun-exposed skin sites; these are tender, red, scaly papules and plaques.
- Sun-damaged skin is less elastic than skin in other areas and develops a dull yellowish hue due to solar elastosis.
- Photo-aged skin has more variable pigmentation than other sites due to freckles, solar lentigines, and hypopigmented and scarred areas. There are often prominent blood vessels (telangiectasia).
The role of ultraviolet radiation in the development of skin cancer
UVR is a major carcinogen. It damages the skin by producing reactive oxygen species (free radicals) that damage proteins, lipids, RNA and DNA. According to the two-hit model, where cancer is a result of accumulation mutations to the DNA, the development of skin cancer depends on an individual’s genetic makeup (particularly their MC1R signalling polymorphisms — that determine skin and hair colour and sun sensitivity) plus two factors.
- UVR causes tumour initiation through mutations in DNA.
- UVR is a tumour promoter and causes progressive tumour growth.
Cutaneous melanoma
- The incidence of melanoma is high in fair-skinned populations living close to the equator and is higher in Australia and New Zealand compared to the UK and Canada where levels of UVR are lower.
- In older adults, melanoma mainly affects the patient's head and neck and is associated with chronic exposure to UVR.
- In younger people, melanoma affects the patient's trunk and extremities, especially in people with many melanocytic naevi (moles). This is thought to be due to earlier exposure to UVR, resulting in sunburns.
Non-melanoma skin cancer
- The highest annual incidence of cutaneous squamous cell carcinoma (SCC) and basal cell carcinoma (BCC) is in Australia and the lowest is in Africa.
- SCC and BCC are more common in fair skin (Fitzpatrick skin phototypes I, II and III) than in darker skin (types IV, V and VI). (See SCC in skin of colour and BCC in skin of colour.)
- Actinic keratoses and SCCs are associated with cumulative sun exposure.
- BCCs are the result of intermittent UVR exposure and sunburn.
- Skin cancer in sun-exposed sites is more prevalent in patients that are immune suppressed, particularly organ transplant recipients.
Most BCCs and SCCs in sun-exposed skin carry ‘UVR signature’ mutations (ie, cytosine to tyrosine transitions at cyclobutane pyrimidine dimers) in tumour suppressor genes (PTCH1 and p53 respectively).
Skin cancers are more common in people with inherited photosensitivity disorders. These disorders include:
- Xeroderma pigmentosum
- Oculocutaneous albinism
- Bloom syndrome
- Trichothiodystrophy
- Rothmund Thomson syndrome.
UVR exposure also increases the risk of:
- Merkel cell carcinoma
- Atypical fibroxanthoma
- Other rarer skin cancers.
Skin cancers due to exposure to ultraviolet radiation



How does ultraviolet radiation affect the eyes?
The eyes are partially protected from sunlight by the brow ridges. Before reaching the retina, reflected UVR is filtered by the cornea, melanin in the iris, aqueous humour, and the lens. UVR causes oxidative damage to mitochondrial DNA in the macular part of the neural retina and the retinal pigment epithelium. UVR can also promote inflammatory cytokines and transcription factors within the eye.
Exposure to solar UVR is associated with:
- Photokeratitis and photoconjunctivitis
- Pterygium
- Cataract, especially cortical cataract
- Age-related macular degeneration
- Ocular malignancies
- BCC — responsible for > 90% of eyelid malignancies
- SCC — the most common malignancy affecting the cornea and conjunctiva
- Melanoma — the most common primary intraocular malignancy.
How does ultraviolet radiation affect the immune system?
Photons of UVR are absorbed by chromophores (atoms that generate colour on a compound) in the epidermis and dermis, triggering an immune response.
- UVR promotes the individual's innate immune response by generating antimicrobial peptides in the epidermis. These peptides protect against pathogens and help with cell growth and repair.
- UVR suppresses acquired immune responses via the stimulation of regulatory T cells, which play a crucial role in maintaining cutaneous homeostasis.
- UVR, especially UVB, induces the production of platelet-activating factor, prostaglandin E2, histamine, and tumour necrosis factor alpha; these cytokines generate a life-long population of suppressor T cells and induce neutrophil-mediated inflammation.
- UVB leads to the synthesis of vitamin D, which can also affect immune function.
Photosensitive skin conditions arising from the failure of the normal immune response include:
- Polymorphic light eruption
- Chronic photosensitivity dermatitis
- Photocontact dermatitis.
- Photoaggravated disorders (eg, cutaneous lupus erythematosus).
Photosensitivity disorders



Other immune-related conditions associated with ultraviolet radiation
Asthma
- People who live at latitudes close to the equator where there is higher UVB have an increased risk of developing atopic asthma. Conversely, they have a lower risk of non-atopic asthma.
Infection
UVR suppresses the acquired immune response to microbial infections. It reduces the protective efficacy of vaccinations. UVR related immunosuppression may reactivate some latent infections and convert asymptomatic infections to symptomatic infections. It can also boost the oncogenic properties of microbes, such as human papillomavirus.
Beneficial effects of ultraviolet radiation
The beneficial effects of UVR include:
- Synthesis of vitamin D2 and D3 in the skin.
- Reduction in cardiac mortality — this may be due to vitamin D synthesis or to lower blood pressure and serum cholesterol.
- Protection against some autoimmune diseases (eg, multiple sclerosis, type 1 diabetes mellitus, and rheumatoid arthritis).
- Reduction in risk of infections (eg, tuberculosis, including cutaneous tuberculosis and viral respiratory tract infections).
- Improved well-being and reduced risk of depression — one theory relates this to increased production and expression of beta-endorphin in keratinocytes.
- Maintenance of healthy circadian cycles through the suppression of melatonin produced by the pineal gland, so reducing the risk of seasonal affective disorder (SAD).