

Acral lentiginous melanoma dermoscopy — extra information
Introduction Clinical features Dermoscopic features BRAAFF algorithm Differential diagnoses Histology
What is acral lentiginous melanoma?
Acral lentiginous melanoma is a type of melanoma arising on the palms of the hands, soles of the feet, or the underside of fingers or toes.
What are the clinical features of acral lentiginous melanoma?
Acral lentiginous melanoma starts as a slowly enlarging flat patch of discoloured skin.
The characteristics of acral lentiginous melanoma include:
- Large size: > 6 mm and often several centimetres or more in diameter at diagnosis
- Variable pigmentation: most often a mixture of brown, and blue-grey, black and red colours
- A smooth surface at first, later becoming thicker with an irregular surface that may be dry or wart-like
- Ulceration or bleeding.



What are the dermoscopic features of acral lentiginous melanoma?
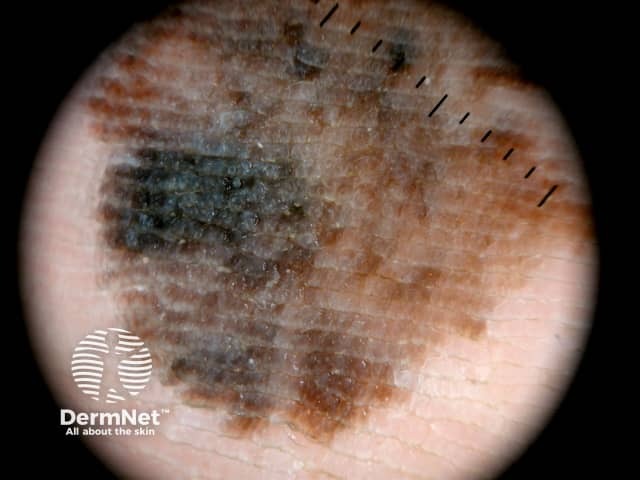
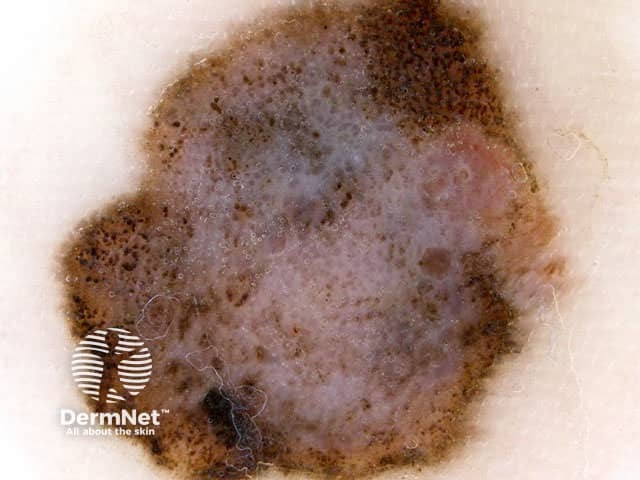
The most frequently observed dermoscopic features of acral lentiginous melanoma are:
- Parallel ridge pattern (furrows remain relatively hypopigmented)
- Asymmetrical structure and colours
- Multicomponent pattern: a combination of many pigmentation patterns
- Diffuse pigmentation of different shades of brown colour not respecting furrows or ridges.





The use of the BRAAFF algorithm in the dermoscopic diagnosis of acral lentiginous melanoma
In this algorithm, one point is required to make the diagnosis of melanoma [1].
- B: blotch, irregular +1
- R: ridge pattern, parallel +3
- A: asymmetry of structures +1
- A: asymmetry of colours +1
- F: furrow pattern, parallel -1
- F: fibrillar pattern -1
Using the BRAAF algorithm to diagnose acral melanoma


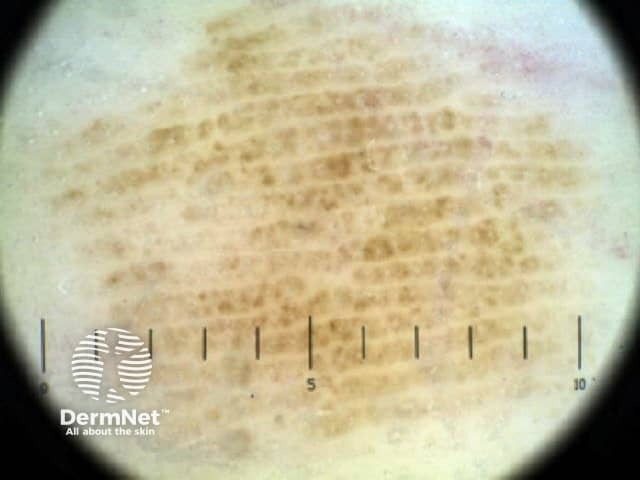
Using the BRAAF algorithm to diagnose acral naevus



What is the dermoscopic differential diagnosis of acral lentiginous melanoma?
It can be clinically and dermoscopically challenging to make the correct diagnosis in pigmented acral lesions. The following are differential diagnoses of acral lentiginous melanoma.
Acral naevus
- Pigmentation on the ridges of the surface skin markings is characteristic of early acral melanoma.
- Pigmentation along the furrows of the skin markings is characteristic of acral naevus.
These dermoscopic patterns are termed the parallel ridge pattern and the parallel furrow pattern, respectively. The sensitivity and specificity of the parallel ridge pattern in diagnosing early acral melanoma is 86% and 99%, respectively. However, dermoscopic features in acral naevus (especially congenital acral naevus) sometimes mimic the parallel ridge pattern [2].
Haemorrhage
The presence of a red-black homogeneous pigmentation, often combined with satellite globules is most likely indicative of haemorrhage. A positive scratch test (where removing a sample of the surface of the skin surface reveals blood) may be considered as an additional diagnostic clue to differentiate from melanoma [3].
Viral wart
Irregular pigmentation at the edge of a warty nodule could be indicative of melanoma [4].
Tinea nigra
Tinea nigra, a superficial fungal infection caused by Phaeoannellomyces werneckii, presents as a hyperpigmented, nonscaling macule of variable size and shape. Typically lacking induration, erythema, or pruritus, these 'ink spot' lesions may resemble junctional naevus or melanoma [5].



What is the histological explanation of acral lentiginous melanoma?
The pathological diagnosis of melanoma can be very difficult. Histological features of acral lentiginous melanoma include an asymmetrical proliferation of melanocytes at the dermo-epidermal junction.
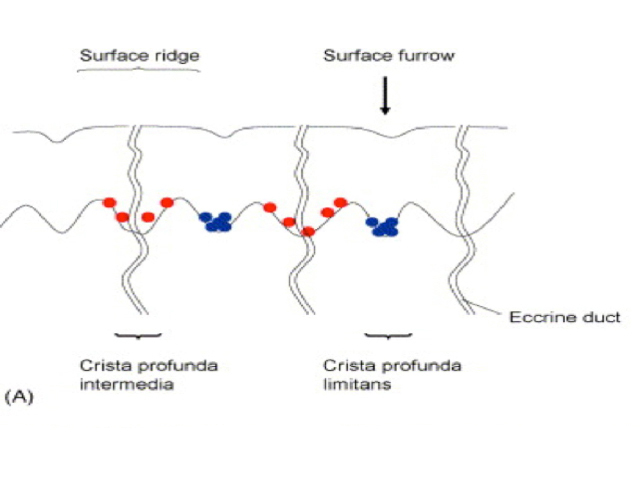
Preferential proliferation patterns of early melanoma cells and naevus cells in acral volar skin. Early melanoma cells (red dots in the diagram below) are mainly found as individual cells in the crista profunda intermedia under the surface ridge. In contrast, nests of acral naevus cells (blue dots in the diagram) are seen in the crista profunda limitans under the surface furrow [6].
References
- Lallas A, Kyrgidis A, Koga H et al. The BRAAFF checklist: a new dermoscopic algorithm for diagnosing acral melanoma. Br J Dermatol 2015; 173: 1041–9. DOI: 10.1111/bjd.14045. PubMed
- Saida T, Koga H, Uhara H. Key points in dermoscopic differentiation between early acral melanoma and acral nevus. J Dermatol 2011; 38: 25–34. DOI: 10.1111/j.1346-8138.2010.01174.x. PubMed
- Zalaudek I, Argenziano G, Soyer HP, Saurat JH, Braun RP. Dermoscopy of subcorneal hematoma. Dermatol Surg 2004; 30: 1229–32. DOI: 10.1111/j.1524-4725.2004.30381.x. PubMed
- Deng W, Yu R, Cui Y, Zheng Z. Amelanotic acral melanoma misdiagnosed as verruca plantaris. An Bras Dermatol 2019; 94: 86–8. DOI: 10.1590/abd1806-4841.20197568. PubMed Central
- Tseng SS, Whittier S, Miller SR, Zalar GL. Bilateral tinea nigra plantaris and tinea nigra plantaris mimicking melanoma. Cutis 1999; 64: 265–8. PubMed
- Takata M, Saida T. Genetic alterations in melanocytic tumors. J Dermatol Sci 2006; 43: 1–10. DOI: 10.1016/j.jdermsci.2006.05.002. PubMed
On DermNet
Other websites