

IgG4-related skin disease pathology — extra information
Introduction Histology Special stains Classification Differential diagnoses
Introduction
IgG4-related disease is a recently described entity. It is characterised by:
- High levels of circulating IgG4 (>135 mg/dL) in 60–70% of patients
- Tissue infiltration of IgG4+ plasma cells
- Fibroinflammatory change in various organs such as the pancreas, salivary, lacrimal, etc
- Striking histological similarities across organs.
Histology of IgG4-related skin disease
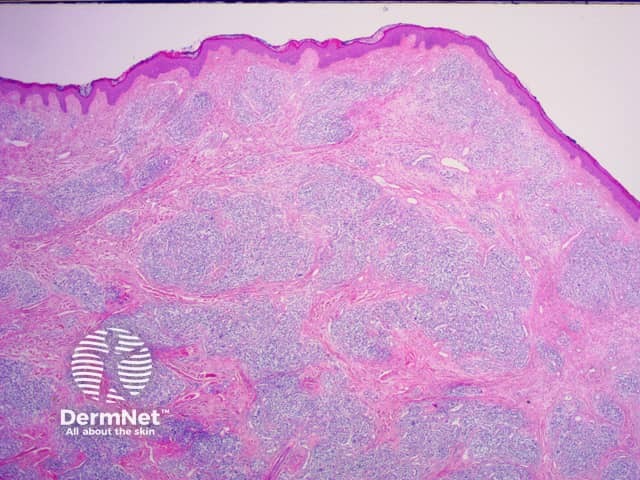
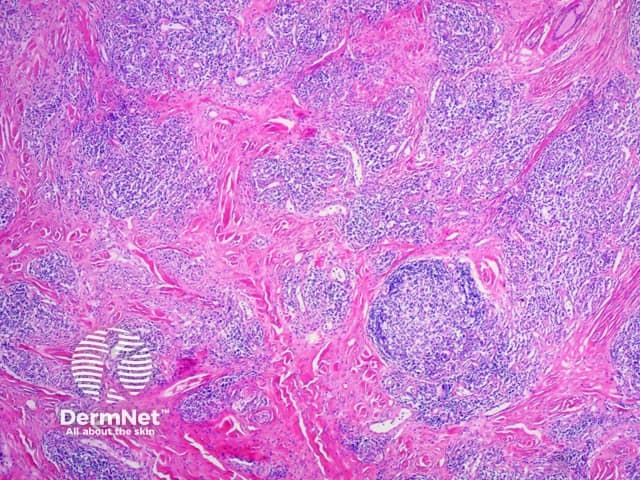
- Dense lymphoplasmacytic infiltrate (figures 1,2)
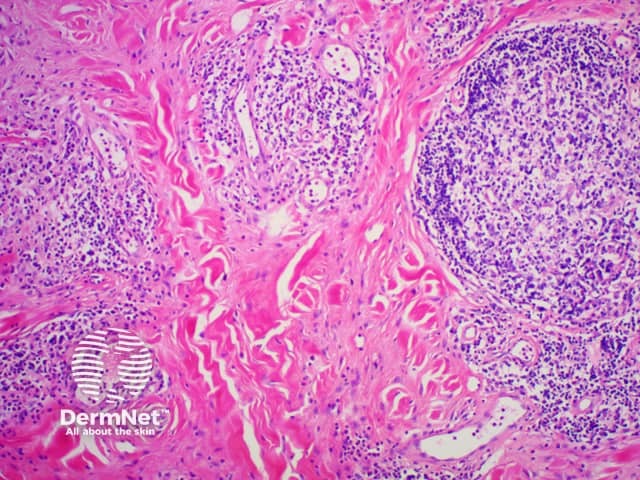
- Storiform fibrosis (fibrosis in a cart-wheel pattern, figure 3)
- Modest-to-moderate tissue eosinophilia (figure 4)
Generally, the minimum for making the diagnosis for most tissues is from 30 to 50 IgG4-positive cells per high power field. However, in some organs or tissues e.g kidney, only 10 IgG4-positive plasma cells per high power field may be sufficient.

Special stains of IgG4-related skin disease
- The CD3 stain illustrates the dense population of T lymphocytes (figure 5)
- The CD20 stain illustrate the population of plasma cells/ B cells (figure 6)
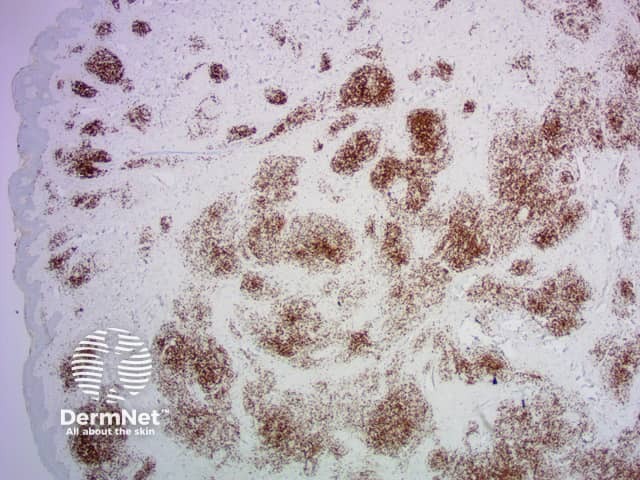
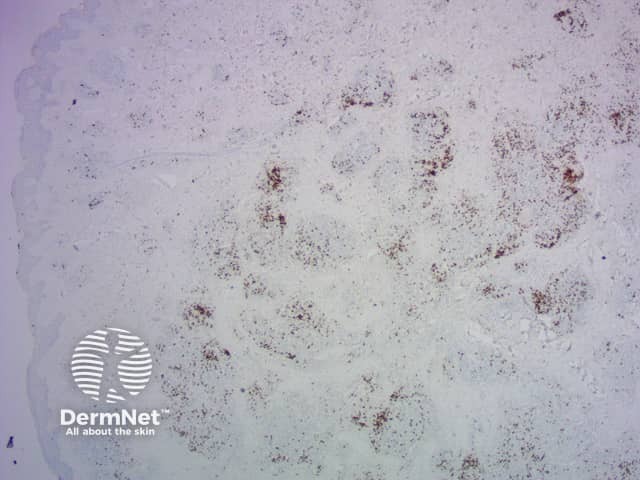
- The anti IgG4 stain which looks brown shows an impressive >250 IgG4 +B cells on high power field (figure 7)

Classification of IgG4-related skin disease
Yokura et al (2014) proposed a classification of IgG4-related skin disease which divides it into primary, mass-forming lesions due to the direct infiltration of plasma cells and secondary lesions which are due to IgG4-mediated inflammation through secondary mechanisms.
Primary lesions include:
- Cutaneous plasmacytosis
- Pseudolymphoma and angiolymphoid hyperplasia with eosinophilia
- Mikulicz disease (inflammation of lacrimal and salivary glands).
Secondary lesions include:
- Psoriasis-like lesions
- Unspecified maculopapular or erythematous lesions
- Hypergammaglobulinaemia, purpura and urticarial vasculitis.
- Ischaemic digit
The diagnostic criteria on histology proposed for skin disease are the following:
- Primary IgG4 related skin disease
- Marked lymphocyte and plasmacyte infiltration, IgG4+/IgG+ >40%
- No of IgG4+ cells per high power field >10.
Secondary IgG4-related skin disease
- Plasmacyte infiltration with IgG4+/IgG+ >40% and/or perivascular IgG4 deposition
Differential diagnosis of IgG4-related skin disease
The differential diagnosis of immunoglobulin G4-related disease (IgG4-RD) is broad and depends upon the specific site of involvement and clinical presentation.
References
- Tokura Y, Yagi H, Yanaguchi H et al. IgG4‐related skin disease. Br J Dermatol. 2014; 171: 959–67. PubMed.
- Masaki Y, kurose N, Umehara H.IgG4-related disease: a novel lymphoproliferative disorder discovered and established in Japan in the 21st century. Journal of clinical and experimental hematopathology 2011; 51(1): 13–20. PubMed.
- Haralampos MM, Fragoulis GE, Stone JH. Overview of IgG4-related diseases. Retrieved from UptoDate on 17/09/15.
On DermNet