

Pityriasis lichenoides et varioliformis acuta pathology — extra information
Pityriasis lichenoides et varioliformis acuta (PLEVA) presents with haemorrhagic papules that resolve to leave varioliform scars. It is usually a self-limiting acute dermatosis. It is also known as Mucha Habermann disease.
Histology of PLEVA
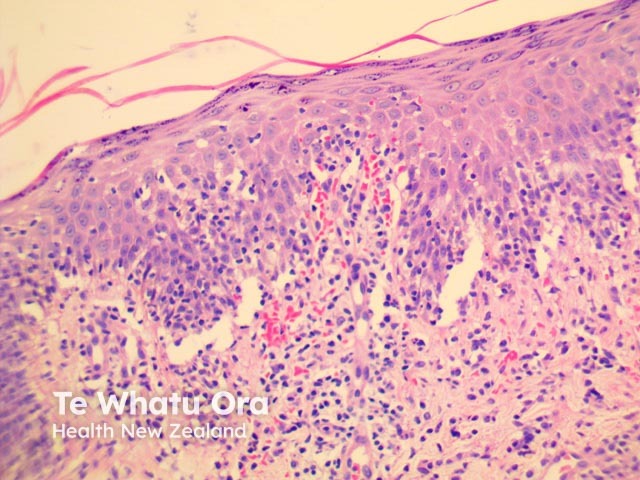
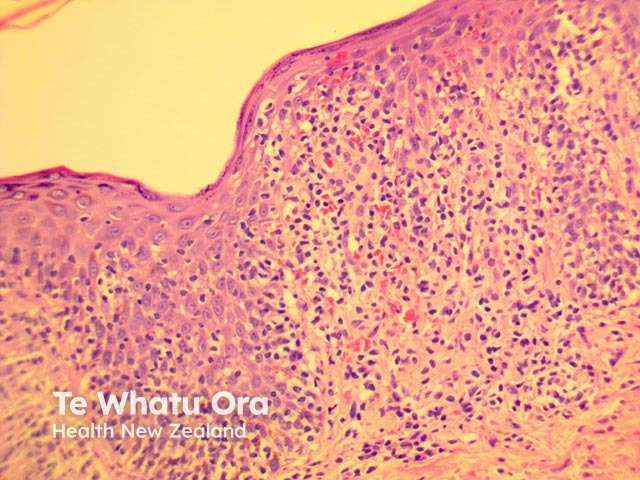
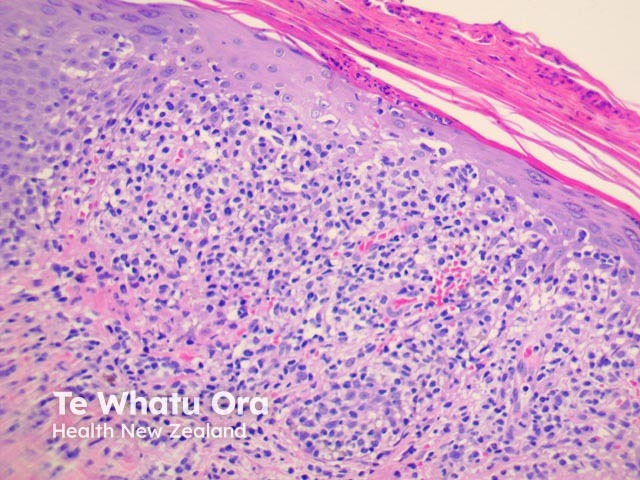
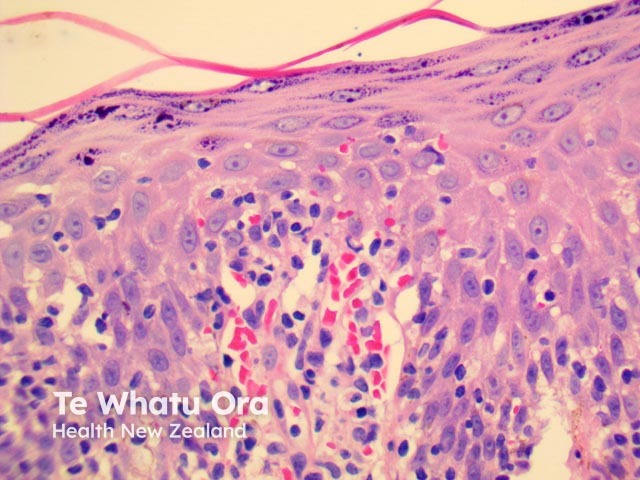
PLEVA has sharply delimited, moderately dense, lymphocytic infiltrate involving the superficial vascular plexus, which extends in a wedge-shaped pattern to involve the lower dermis (figure 1). The superficial dermis shows a dense lichenoid infiltrate and impressive exocytosis of lymphocytes into the epidermis. The overlying stratum corneum shows parakeratosis which may be confluent and contain collections of neutrophils (figure 2). The epidermis shows pronounced hydropic change and foci of keratinocyte necrosis. Scattered extravasated erythrocytes are seen (figure 3).

Images provided by Dr Duncan Lamont, Waikato Hospital
Special studies in PLEVA
None are generally needed. Immunoperoxidase studies have shown the lymphocytic infiltrate consists of CD8/cytotoxic T cells.
Differential diagnosis of PLEVA
Cutaneous T-cell lymphoma
Lymphocytic vasculitis
References
- Weedon’s Skin Pathology (Third edition, 2010). David Weedon
On DermNet