

Juvenile xanthogranuloma pathology — extra information
Introduction
Histology
Special studies
Differential diagnoses
Introduction
Juvenile xanthogranuloma usually presents in young children as a smooth pink or yellow nodule.
Histology of juvenile xanthogranuloma
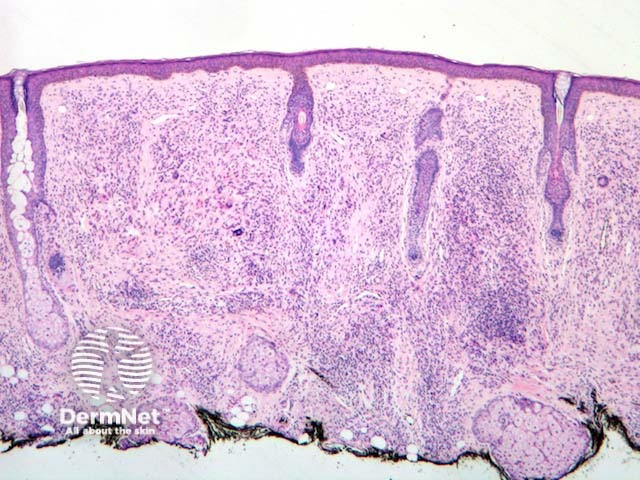
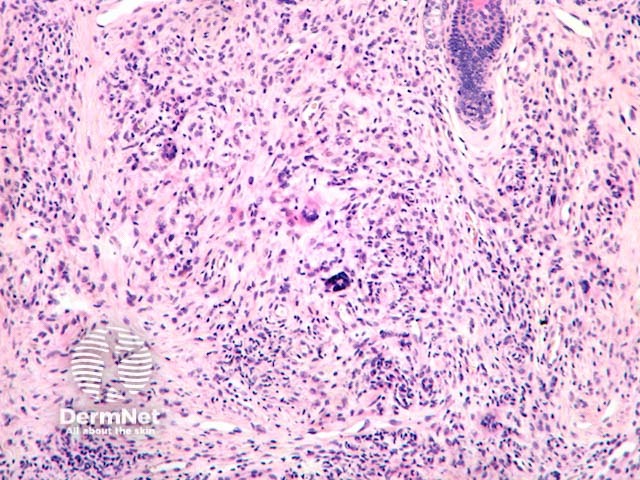
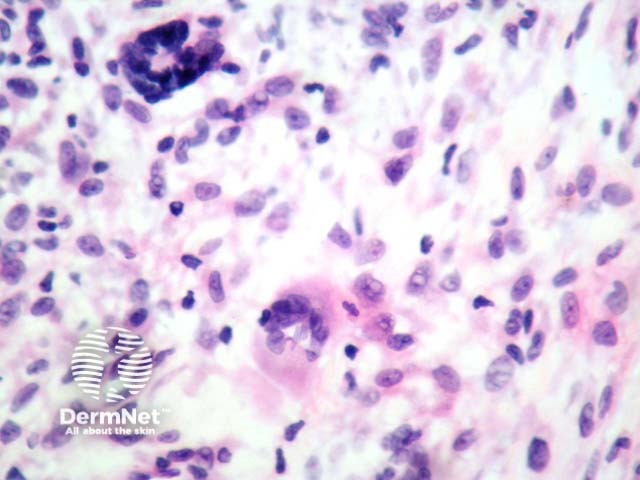
In juvenile xanthogranuloma, the lesion begins as a dense lymphohistiocytic proliferation of dermis with rare giant cells. As it evolves, the dermal tumour contains a population of foamy histiocytes and giant cells (figures 1–3). Touton giant cells are quite characteristic of juvenile xanthogranuloma (best seen in figure 3). These cells contain a ring of nuclei surrounding a central homogeneous cytoplasm, while foamy cytoplasm surrounds the nuclei. Later the cells become more spindled and fibrohistiocytic-like.
Special studies for juvenile xanthogranuloma
Immunohistochemistry can be used. Typically the tumour is positive with CD68, alpha-1-antichymotrypsin, lysozyme, vimentin, and Factor XIIIa. Useful negative stains include S100 and CD1a.
Differential diagnosis for juvenile xanthogranuloma
- Dermatofibroma typically lacks Touton giant cells and has a dense collagenous stroma, storiform growth pattern, and often an overlying pseudoepitheliomatous hyperplasia.
- Xanthomas show more uniform foamy histiocytes and more frequently occur in multiplicity. the polymorphous infiltrate typically seen in juvenile xanthogranuloma is usually absent.
- Langerhans cell histiocytosis typically shows staining with S100+ and CD1a+.
- Reticulohistiocytoma is composed of histiocytes with eosinophilic or ground glass cytoplasm.
References
- Langerhans cell histiocytosis — PathologyOutlines.com
On DermNet
Other websites
- Juvenile xanthogranuloma — PathologyOutlines.com