Introduction Histology Special stains Histology Differential diagnoses
The two primary cutaneous amyloidoses lichen and macular amyloidosis show similar histological features and so are described together.
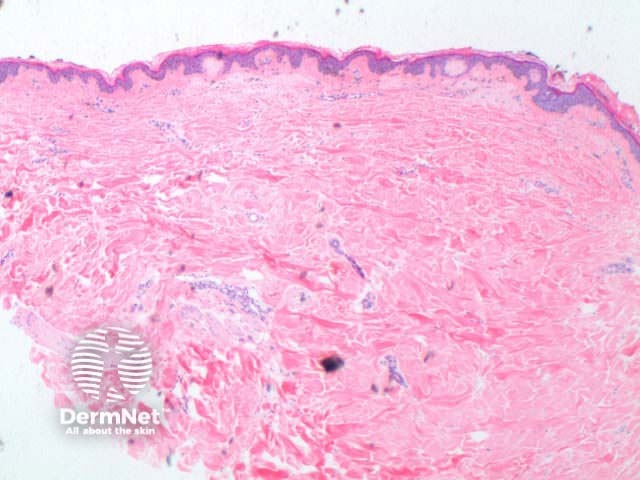
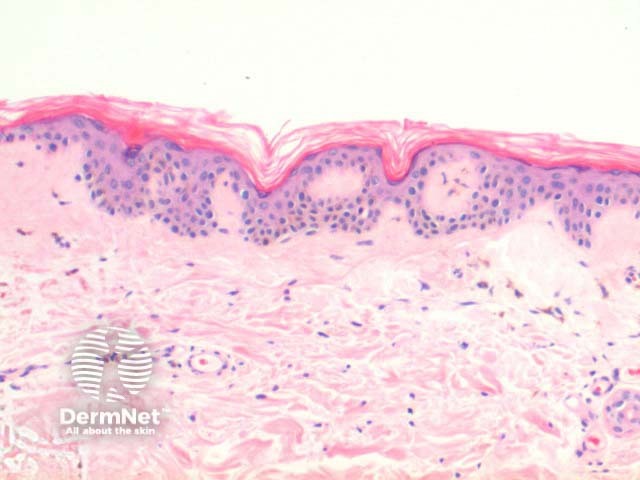
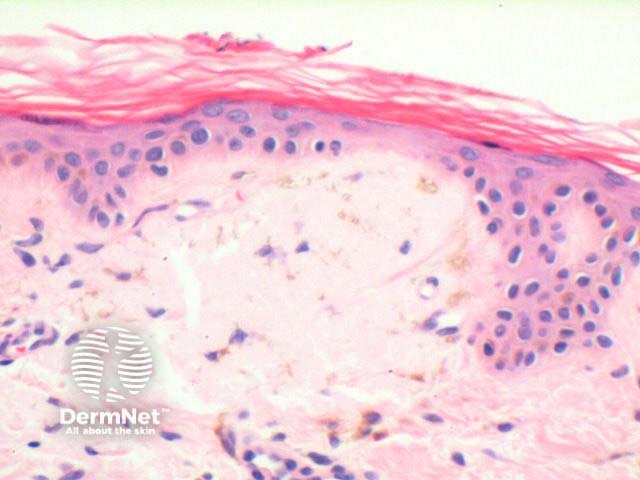
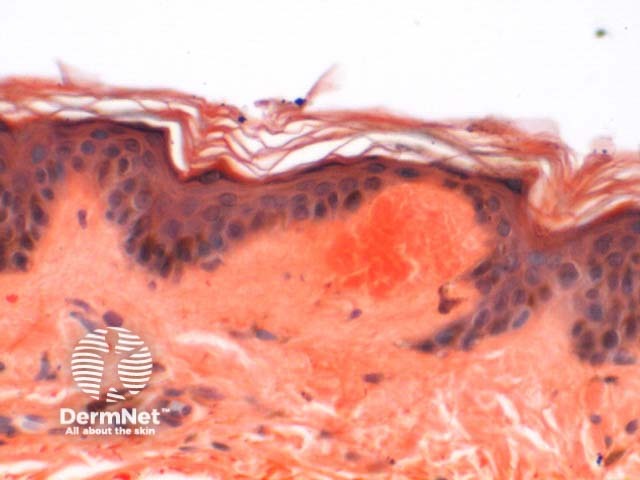
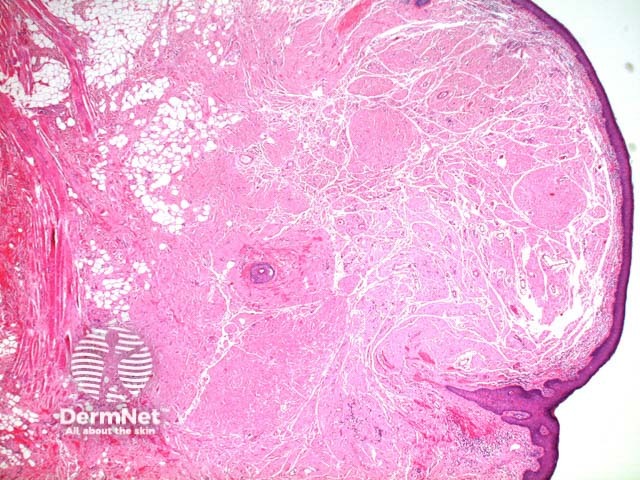
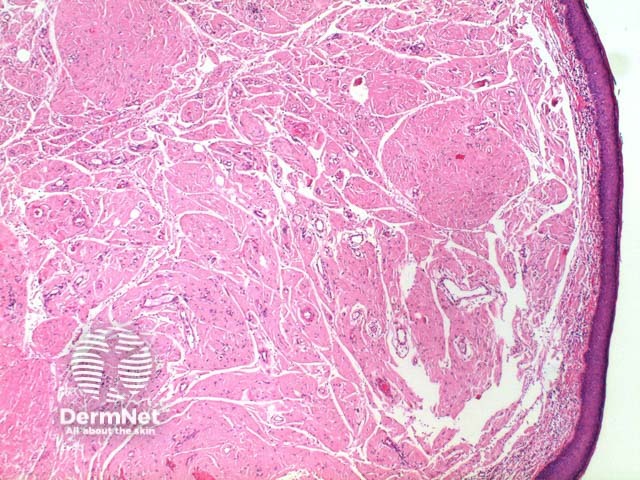
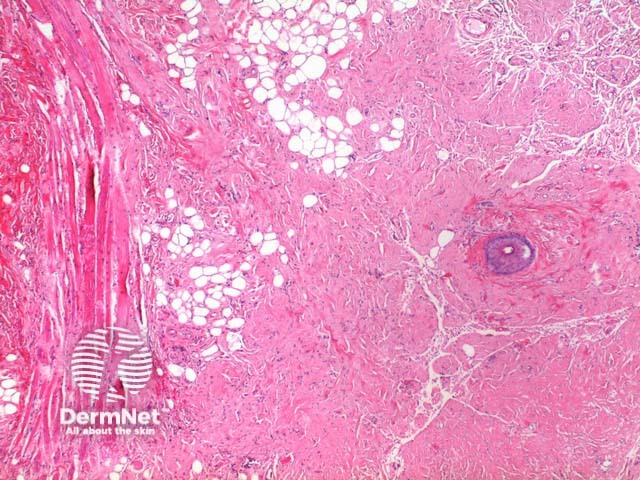
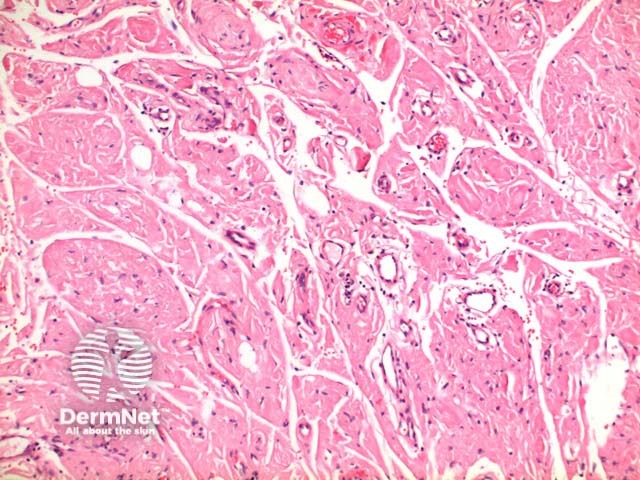
The scanning power view of primary cutaneous amyloidosis can be relatively unremarkable (figure 1). The key component of the histology is the deposition of pink amorphous material within the papillary dermis. This forms a number of scattered and confluent globular deposits (figures 2, 3, 4). There is increased pigmentation of the basal layer and a scattered melanophages in the papillary dermis (figure 4). The deposited material is identical in both macular and lichen amyloidosis, the difference is in the epidermal appearances. In lichen amyloidosis, there is hyperkeratosis and epidermal hyperplasia which can range from mild to marked thickening (figure 2). There may also be mild papillary dermal fibrosis. This is in keeping with the chronic excoriation underlying this condition, and the histological overlap with lichen simplex chronicus.

Congo-red highlights the deposits, and under polarization takes on a bright apple-green birefringence (figure 5). There are significant limitations in the special stains for this condition. A positive reaction with this stain is not always readily seen, and false negatives not infrequently occur.
Other less frequently used stains for cutaneous amyloid include crystal violet, pagoda red and methyl violet.
Cytokeratin (CK) staining can be used to identify the amyloid as epidermal in origin. Positive staining with immunostaining to kappa and lambda light chains is suggestive of AL amyloid deposition and should prompt consideration of systemic amyloidosis.
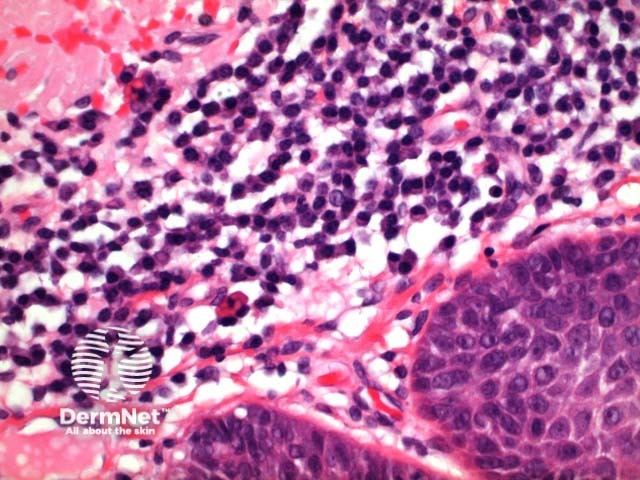
The scanning power view reveals a tumoral deposit within the dermis (figure 6). This may extend into the subcutaneous tissue (figures 7, 8, 9). Prominent clefting can be seen making superficial cases difficult to differentiate from colloid milium and paracolloid. The presence of numerous plasma cells in the accompanying inflammatory infiltrate, commonly with scattered Russell bodies, is helpful (figure 10).
Primary cutaneous amyloidosis should be considered when faced with minimal pathological changes, aptly named an ‘invisible dermatosis’. The cutaneous amyloid deposits can easily be overlooked when not looked for specifically.
Colloid milium and paracolloid: colloid milia are typified by superficial deposits of acellular amorphous material with prominent clefting. Paracolloid (colloid degeneration) may extend more deeply, with more subtle clefting, and has a more basophilic colour. Both entities are typically congo red negative while keratin antibody positive.

