

Eruptive xanthoma pathology — extra information
Introduction Histology Special studies Differential diagnoses
Introduction
Eruptive xanthoma presents as crops of pink papules which are often pruritic. It occurs as a result of high concentrations of plasma triglycerides. Many patients have uncontrolled diabetes. The xanthomas usually disappear when the underlying condition is treated.
Histology of eruptive xanthoma
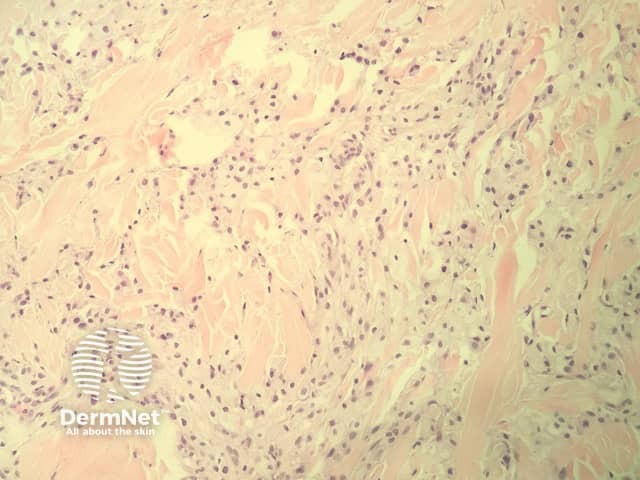
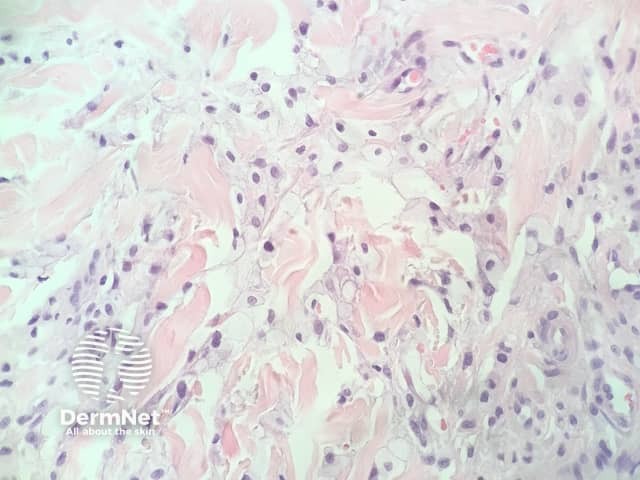
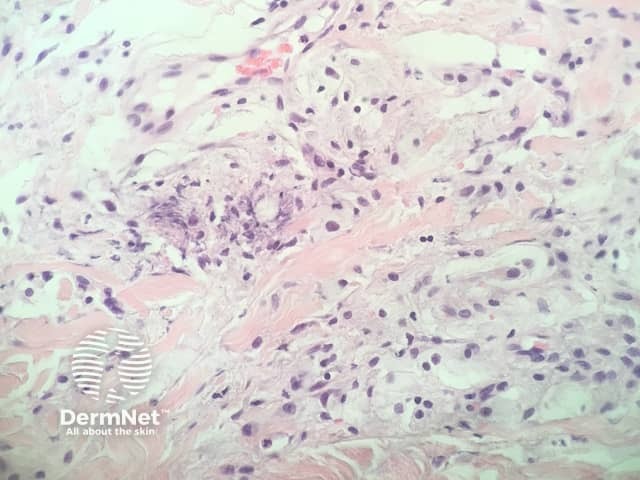
In eruptive xanthoma, the dermis contains a dense population of foamy histiocytes (histiocytes filled with lipid material as well as extracellular lipid (figures 1–3). There is often an associated acute and chronic inflammatory response (figure 4).

Special studies for eruptive xanthoma
None are generally needed. Special stains to highlight lipid deposition have been described but are rarely needed.
Differential diagnosis for eruptive xanthoma
There are a wide range of conditions which result in the accumulation of foamy histiocytes in the dermis and may mimic eruptive xanthoma. The correct diagnosis is generally confirmed by correlating the features of the biopsy with the clinical presentation and serologic findings.
Other xanthomatous conditions include:
- Infection — the pathology of leprosy may show an accumulation of foamy histiocytes in the dermis. Special stains for the causative organisms (Mycobacterium leprae) can be useful in difficult cases
- Other xanthomas — these are usually easily excluded with the clinical presentation. It is unusual in other forms of xanthoma to see the degree of extracellular lipid and acute inflammatory response seen in eruptive xanthoma
- Xanthogranuloma — these typically show a mixture of inflammatory cells, and characteristically show Touton giant cells.
References
- Kala J, Mostow EN. Images in clinical medicine. Eruptive xanthoma. N Engl J Med 2012; 366: 835. doi: 10.1056/NEJMicm1105301. Journal
On DermNet
Other websites
- Xanthoma — PathologyOutlines.com
- Xanthogranuloma — PathologyOutlines.com