

Basic photophysics
Created 2007.
Learning objectives
- List lamps that produce ultraviolet radiation for phototherapy
- Describe a fluorescent source of UV radiation
- Explain variation in output of a fluorescent source or UV radiation
- Recognise specific spectral output curves for BB-UVB, NB-UVB, PUVA lamps, UVA1
- Describe what is meant by dosimetry
- Name radiometric terms and units are used for UVR dosimetry.
Introduction
The following table lists some basic photophysics definitions.
| Phototherapy | The use of non-ionising portions of the electromagnetic spectrum for its therapeutic effect. It may involve partial or whole-body exposure. |
| Radiation | The transfer of energy by particles or waves that can travel across a vacu |
| Ionising radiation | Those forms of radiation that have sufficient energy to displace electrons from atoms. These include: alpha particles, beta particles, gamma rays, x-rays and neutrons. |
| Non-ionising radiation | Those forms of radiation that do not have sufficient energy to displace electrons from atoms. It is classified as follows: ultraviolet radiation; visible light; infrared radiation; microwave radiation; radio frequency radiation; extreme low frequency (ELF) electromagnetic fields. |
| Fluorescence | Emission of light produced by certain substance when excited by UVR. This emission ends when UV source is removed. |
| BL (Black Light) | Lamp that produces 365nm with visible light. |
| BLB (Black Light Blue) | Lamp that produces 365 nm without visible light, commonly called ‘Black light’ or ‘Wood's light’. |
In dermatology, the term phototherapy is usually applied to the use of ultraviolet (UV) radiation in the treatment of skin diseases, to be considered in this topic. However ‘phototherapy’ may sometimes apply to visible light, used in lasers and flash lamp sources, and infrared radiation (generally referred to as ‘heat lamps’).
Applications for ultraviolet radiation in medicine include:
- UVC in laboratories and kitchens as a bactericidal agent and for various diagnostic and research applications
- UVB for phototherapy using broadband and narrowband sources
- UVA used alone or with topical or oral photosensitisers such as 8-methoxypsoralens (8-MOP PUVA); Wood's light for diagnosis of fluorescing skin diseases and identification of pigmentary disorders.
- Extracorporeal photopheresis, in which circulating leucocytes are exposed to 8-MOP PUVA.
Photodynamic therapy refers to the combination of a photosensitising agent, oxygen and exposure to visible light to cause a selective destruction of abnormal tissue.
Lamps producing UV radiation
Lamps producing UV radiation include:
- Mercury discharge lamps
- Mercury vapour arcs
- Metal halide lamps
- Xenon arc lamp
- Diodes
- Excimer lasers
Original heliotherapy bulbs

The original mercury discharge lamps produced 90% of its energy as a band of UVC, at 254nm. This is high energy, so causes a lot of damage to superficial skin but it doesn't penetrate deeply and is not useful therapeutically.
Fluorescent lamps are low-pressure mercury discharge lamps with a phosphor coating inside the tube. Electrons from the power source excite the mercury atoms to produce UVC, which is then re-emitted by the phosphors as longer wavelengths. Differing phosphors and filters result in lamps with differing and continuous spectral outputs, i.e. primarily UVB, UVA or visible light.
Although ‘heliotherapy’ lamps were introduced in the 1920s, phototherapy became much more practical after the 1960s when powerful fluorescent UV lamps providing a large field size were developed. They proved affordable, reliable, enduring and cool enough to tolerate. Fluorescent bulbs are available in 2-foot and 6-foot lengths, long enough for whole body exposures.
2-foot bulbs
However, fluorescent lamps tend to produce a variable output. The output is less at the top and bottom of the bulb. There is a warm-up time and the bulbs reduce output slowly as they age. It is therefore important to carefully and continuously measure the output in each phototherapy unit to ensure accurate doses are delivered to patients. The bulbs should all be replaced after 500 to 1000 hours of use.
High output metal halide discharge phototherapy machines are also available. Excimer lasers (308nm) are showing promise for treating localised psoriasis but they are very expensive machines.
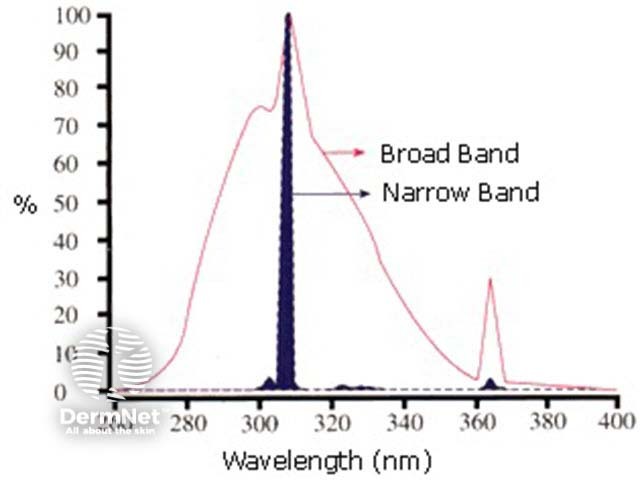
Spectral outputs
Broadband UVB units have been designed to have minimal UVC content using a filter. Although the peak waveband is the same as a narrowband unit, there is considerable additional energy as UVB and as UVA.
UVB at 311-313nm has been demonstrated to be the most efficient waveband for effective clearance of psoriasis. The entire broadband spectrum will cause erythema (burning), so that only a relatively small dose of the effective energy can be delivered before the patient's skin begins to go red. A narrowband unit (TL-01 lamps) produces nearly all its energy as 311-313nm so that more effective treatment can be delivered without injury.
Psoralen interacts with UVA to produce a therapeutic effect, maximal at about 330nm. Fluorescent bulbs used for UVA phototherapy peak at around 360 nm. Standard exposure to UVA on its own has little effect on psoriasis or other skin diseases. Hence standard UVA bulbs are mostly used for photochemotherapy (PUVA).
Recently high output UVA1 bulbs have become available. The name refers to the selection of a relatively narrow band of longer wavelengths peaking at 370nm. The deep penetrating energy has been shown to be effective for atopic dermatitis and scleroderma, and is under investigation for other indications.
Cosmetic applications of UVR, i.e. tanning booths or sun beds, became popular in the 1970s when fluorescent bulbs producing UVA became commercially available. The lack of UVB made them apparently safer to operate and they continue to be widely promoted. Many sun bed operators provide ‘booster’ bulbs that produce significant UVB and a large variety of bulbs are available for cosmetic purposes.
Dosimetry
The measurement of the radiation dose is known as the dosimetry.
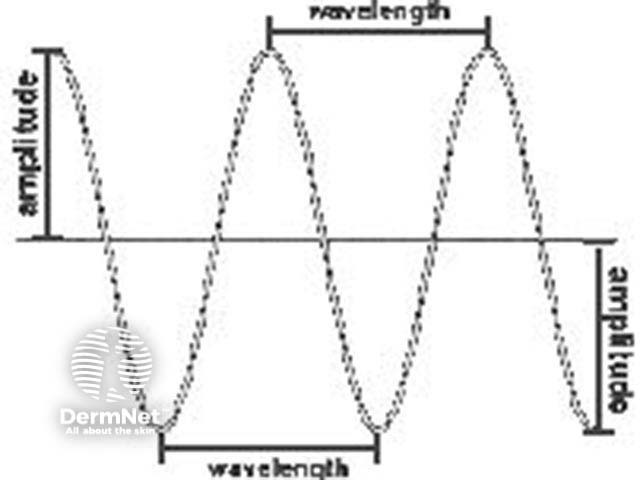
To describe the radiation emitted by a lamp it is necessary to give the distribution of energy as a function of wavelength. Wavelength is the distance between two corresponding points on successive waves.
Radiation detectors (sensors) are sensitive to a limited range of wavelengths, i.e. UVB sensors may measure correctly only at 310nm, and UVA sensors at 350nm. A sensor designed for a specific situation (e.g. to measure irradiance in the UVB cabinet) cannot be used in another (e.g. sunlight) to indicate a safe dose.
Modern electronic phototherapy units have built-in or integrated dosimetry. Sensors detect the output of the lamps, and radiance fluctuations are integrated into the calculated dose. However backup timers are wise and regular recalibration is essential.
There are a variety of different ways of measuring UVR. The technology is complex and will not be covered in this course.
Terminology
Radiometric terms and units are used for UVR dosimetry.
- Radiant energy: the beam of radiation passing through space
- Radiance: the radiation emitted by a source
- Irradiance: the radiation striking the object e.g. patient
- Radiant exposure: the time integral of the irradiance or dose
| Term | Unit | Symbol |
|---|---|---|
| Wavelength | nm | l |
| Radiant energy | J | Q |
| Radiant flux | W | f |
| Irradiance | W/cm2 | E |
| Dose | J/cm2 | H |
One Joule = One watt/sec
Staff safety
Staff working in a phototherapy unit must be protected from exposure to UV radiation.
- Wear wrap-around UV-protective glasses blocking to at least 360nm
- Wear sunscreen on exposed skin
- Attend regular training sessions
UVB burns to unprotected nurse

In addition, there are legal responsibilities regarding the electrical safety of electrical installations (Electricity Act 1992), the training of staff and hazard identification (Health and Safety in Employment Act 1992). An electrician must check devices used to treat patients every 6 months.
Troubleshooting
Common problems include non-functioning lamps, non-functioning ballasts, blown fuses, misplacement of lamps (e.g. UVB instead of UVA). The results may be under- or over-treatment, which could result in severe burns. Ensure all lamps are functioning prior to each treatment and monitor treatment times and meter readings.
Activity
Draw diagrams of the spectral outputs of fluorescent broadband UVB, narrowband UVB, UVA and UVA1 lamps.
References
- Phototherapy resources
- Diffey BL. Sources and measurement of ultraviolet radiation. Methods 2002; 28: 4-13.
- Guidelines for dosimetry and calibration in ultraviolet radiation therapy: a report of a British Photodermatology Group workshop
On DermNet
Information for patients
Books about skin diseases
See the DermNet bookstore