Introduction Clinical features Dermoscopic features Differential diagnoses Histological explanation
Amelanotic melanoma is a form of melanoma in which the malignant cells produce little to no pigment.
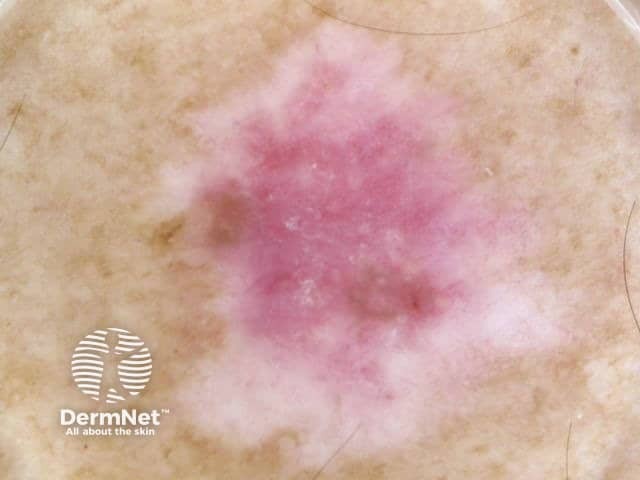
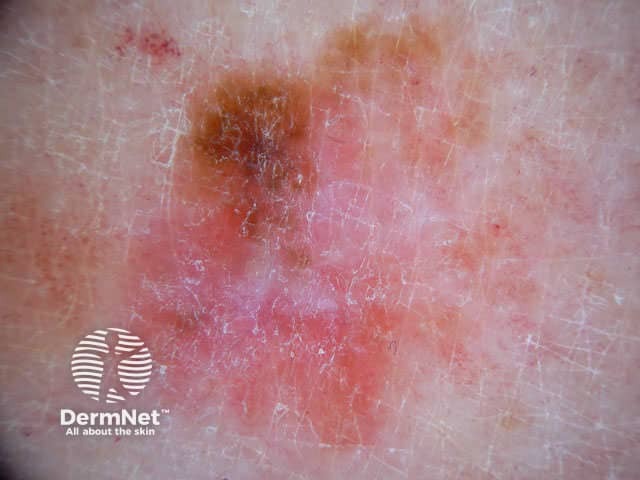
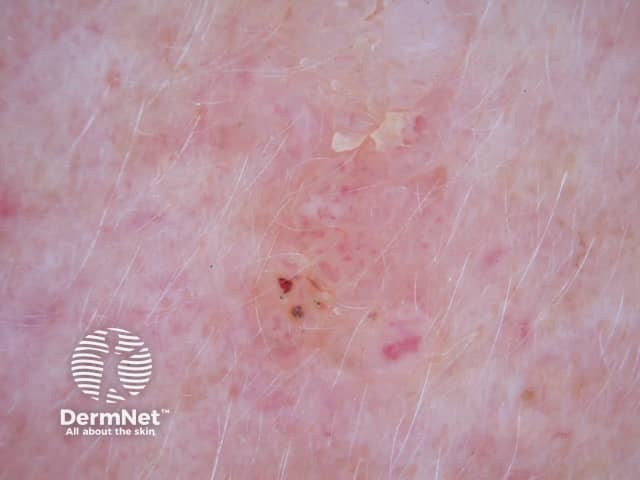
Amelanotic melanomas are classically described as skin coloured. A significant proportion of melanomas are red or pink. Typical early lesions present as asymmetrical macules that may be uniformly pink or red and may have a faint light tan, brown, or grey pigmentation at the periphery. The borders may be well or ill-defined. Use of the 3 R’s (Red, Raised, Recent change), may help screen for amelanotic melanoma.



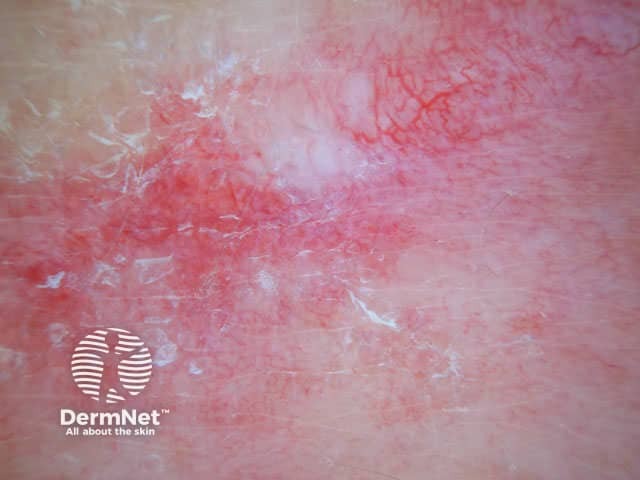
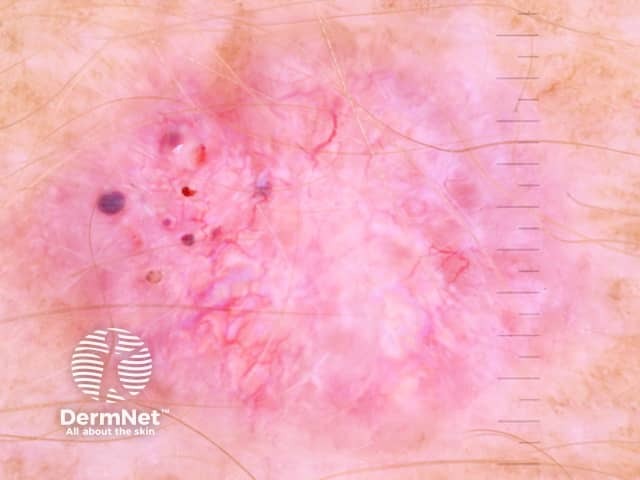
The dermoscopic features of amelanotic melanoma may include:
Vessel morphology should be evaluated carefully if lesions are lacking pigmentation. In the 5 + 2 list below, the presence of a certain type of vessel is asked for; if the answer is “no”, proceed to the next question.
If question number 5 is answered in the affirmative (ie, point-like or loop-like vessels are present), evaluate the absence of white halos and presence of traces of melanin. If “yes,” suspicion of melanoma is raised. Traces of brownish melanin, which may not be visible clinically, present focally within the lesion support the diagnosis of melanoma or Spitz nevus. It can be very difficult to discriminate between amelanotic melanoma and Spitz naevus by dermoscopy. Lesions with point-like or loop-like vessels without white halo must be considered suspicious and removed [1].



Other non-pigmented tumours include:






Histopathologically, an amelanotic melanoma is usually composed of highly malignant epithelioid cells. These cells display pleomorphism, mitotic activity, enlargement, large nucleoli, and lack of maturation as the cells descend into the dermis.

