

Granuloma annulare pathology — extra information
Histology Histological variants Special stains Differential diagnoses
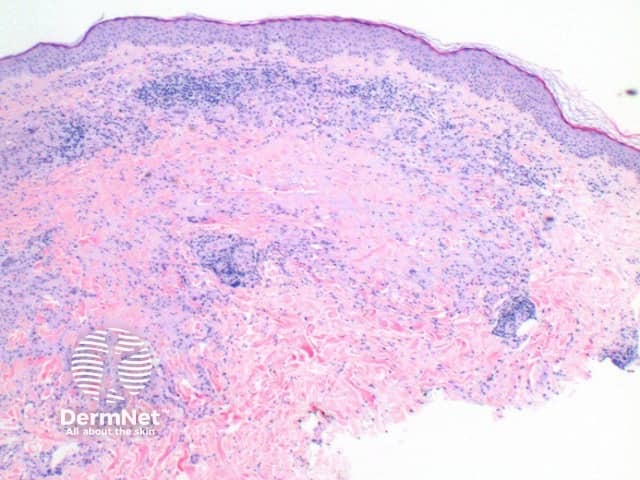
Histology of granuloma annulare
The scanning view of the histology of granuloma annulare shows a granulomatous inflammatory pattern situated within the superficial and mid dermis.
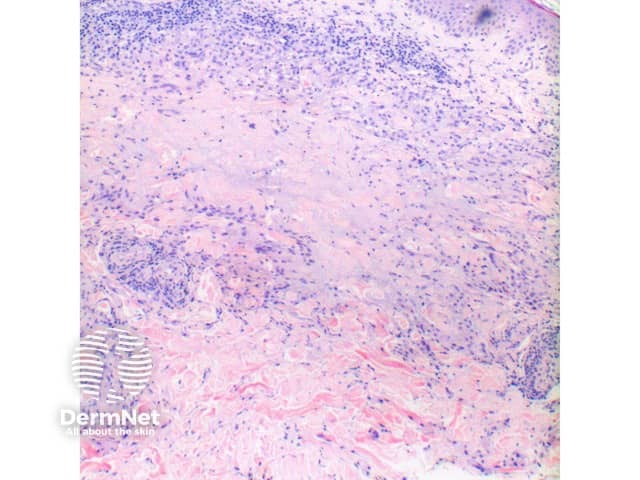
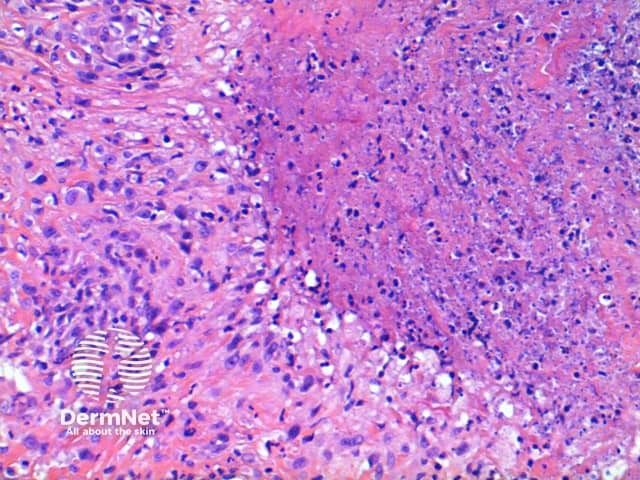
- Figure 1. Closer inspection reveals palisading of histiocytes around a focus of necrobiosis and increased mucin deposition.
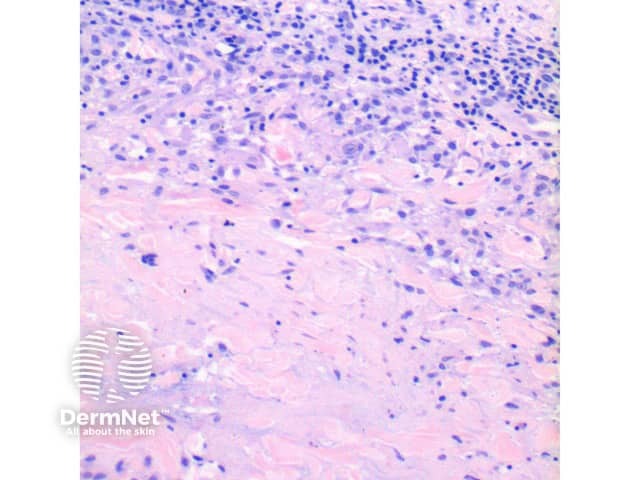
- Figure 2, Figure 3. The intervening dermis appears normal. Multinucleated giant cells are frequently seen.
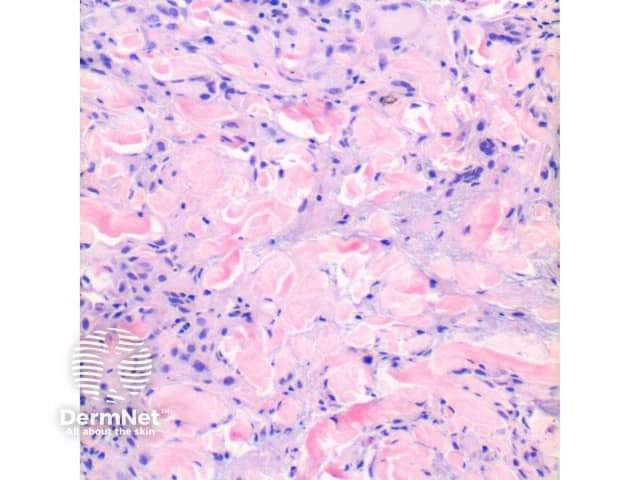
- Figure 4. A mild perivascular and interstitial lymphocytic infiltrate may be seen in the surrounding dermis with scattered neutrophils and eosinophils. Plasma cells are rare.
- Associated vascular fibrin deposition and nuclear dust suggestive of vasculitis appears to be a rare finding.
Histological variants of granuloma annulare
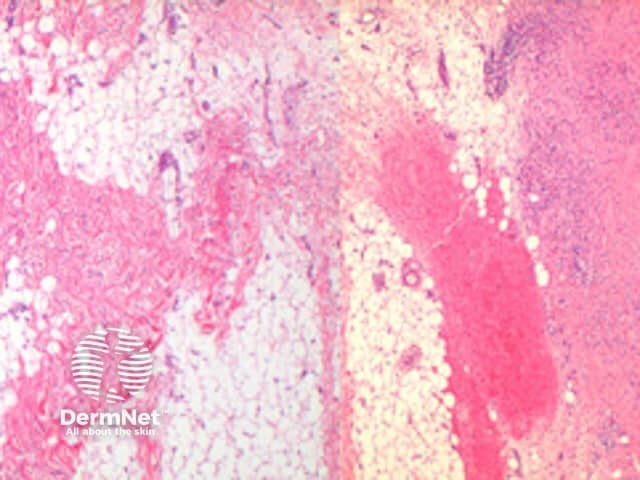
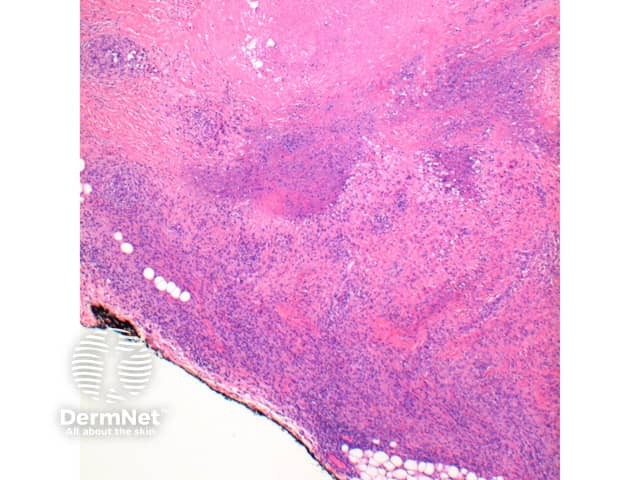
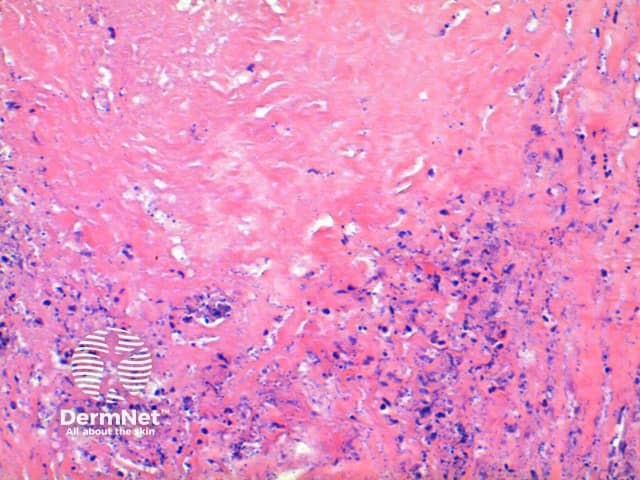
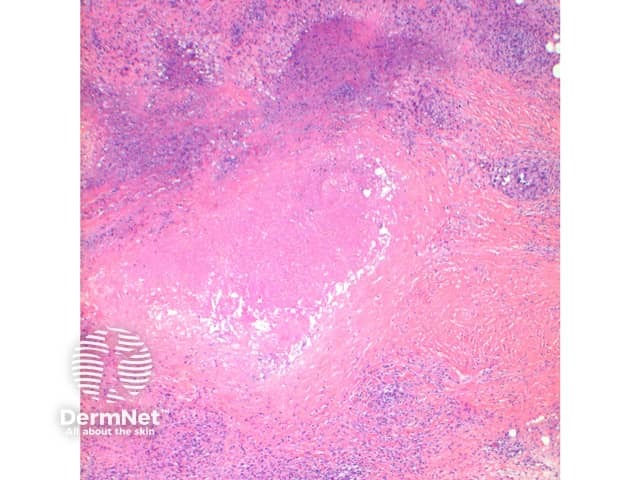
Subcutaneous GA: In this variant the inflammatory infiltrate is predominantly within the deep dermis and extends into the subcutaneous tissue (Figure 5, 6). Large areas of necrobiosis can be seen along with increased numbers of eosinophils (Figures 7, 8, 9).
Mitotically active variant: While typically mitotically activity is low, there is recognised a mitotically active variant which may otherwise raise concern about a proliferative lesion. Caution in these cases is advised to exclude epithelioid sarcoma as discussed below.
Perforating GA: Here the inflammatory infiltrate can be seen to be eliminated through the epidermis via a channel formed between epidermal downgrowths.
Disseminated GA: While the histology may be identical to typical GA, the infiltrate may be sparse and retained within the papillary dermis. Lichen nitidus is sometimes considered in these cases.
Interstitial GA: The low power pattern is different, showing a 'busy dermis' and lacking the necrobiotic and mucinous foci. High power reveals the interstitial infiltrate of benign appearing histiocytes. While less conspicuous, increased mucin is frequently seen around the inflammatory infiltrate. In the presence of many eosinophils and interface changes an interstitial granulomatous drug reaction should be considered.
Special stains in granuloma annulare
Mucin stains such as colloidal iron and alcian blue may be used to highlight the increased connective tissue mucins.
Differential diagnosis of granuloma annulare
Necrobiosis lipoidica: Layered with open ended necrobiotic foci. Lacks mucin. Increased numbers of plasma cells may be a clue.
Rheumatoid nodule: The changes seen here are most similar to the subcutaneous variant of GA. Discriminating features seen in the rheumatoid nodule includes the presence of larger areas of eosinophilic necrobiosis, and a lack of mucin deposition. Clinical history is usually informative.
Epithelioid sarcoma: Always think twice when diagnosing GA on the digits. While the low power pattern may be similar due to the eosinophilic areas of necrosis, closer inspection will always reveal an atypical infiltrate. Immunohistochemistry is definitive in difficult lesions showing Epithelial membrane antigen (EMA) and Cytokeratin (CK) positivity.
References
- Skin Pathology (2nd edition, 2002). Weedon D
- Pathology of the Skin (3rd edition, 2005). McKee PH, J. Calonje JE, Granter SR
On DermNet
Books about skin diseases