

Key clinical-trial evidence for ixekizumab — extra information
Introduction
Clinical trial experience
Adverse event results
Future directions
Introduction
Ixekizumab (Taltz®) is a humanised monoclonal immunoglobulin G antibody developed by Eli Lilly and Company that has been approved in the USA (March 2016) and Europe (April 2016) as a treatment for plaque psoriasis.
Ixekizumab is a specific inhibitor of interleukin-17A (IL-17A), a pro-inflammatory cytokine that has a role in the development of several inflammatory conditions including psoriasis.
The efficacy of ixekizumab as a treatment for moderate to severe plaque psoriasis has been evaluated in three randomised placebo-controlled trials, UNCOVER-1, UNCOVER-2 and UNCOVER-3. UNCOVER-2 and UNCOVER-3 also compared ixekizumab to etanercept.
Clinical trial experience
UNCOVER-1: efficacy and adverse reactions
Uncover-1 was a prospective, double-blind, multicentre trial that consisted of 1296 patients randomly distributed in a 1:1:1 ratio to receive 80 mg ixekizumab every two weeks (Q2W), 80 mg ixekizumab every four weeks (Q4W), or placebo, respectively.
- Patients in the ixekizumab groups received a single 160 mg starting dose at week 0 followed by 80 mg Q2W or Q4W.
- All patients were given two subcutaneous injections (ixekizumab or placebo) at week 0 and one subcutaneous injection (ixekizumab or placebo) at week 2, 4, 6, 8, and 10.
- In this study, the co-primary efficacy endpoint at 12 weeks was a 75% improvement in the composite Psoriasis Area Severity Index (PASI) score and at least a 2-point increase from baseline in the static Physician's Global Assessment (sPGA) 0 or 1.
- PASI measures the extent and severity of psoriasis by assessing average redness, thickness and scaliness of skin lesions (each graded on a zero to four scale), weighted by the body surface area of involved skin.
- The sPGA is the physician's assessment of the severity of a patient's psoriasis lesions overall at a specific point in time and is a necessary measure the FDA uses to evaluate effectiveness.
- 89.1% and 82.6% of patients treated with ixekizumab once every 2 (n = 433) or 4 (n=432) weeks, respectively for 12 weeks, achieved an improvement in PASI of ≥75% (PASI 75) compared to 3.5% of placebo recipients (n = 431; p < 0.001 for both ixekizumab regimens vs placebo).
- The percentage achieving sPGA 0 or 1 was 81.8% and 76.4% for ixekizumab Q2W and Q4W, respectively, compared to 3.2% in those who took a placebo (P < 0.001 vs placebo).
- After 12 weeks, patients who responded to ixekizumab were randomised to 48 weeks treatment with ixekizumab 80mg every 4 (n = 229) or 12 ( n= 227) weeks or placebo (n = 226).
- At week 60, sPGA of 0 or 1, PASI 75 and PASI 100 were maintained in 72.9, 77.7 and 52% of ixekizumab recipients, respectively.
- The most common (> 1%) adverse events were nasopharyngitis, erythema and pain at the injection site.
- The proportions of patients with a candida infection at 12 weeks were 0.9% and 0.6% for ixekizumab Q2W and ixekizumab Q4W, respectively, compared to 0.5% for placebo.
- Adverse event comparisons are not statistically significant, as the study was powered to detect differences in efficacy rather than rates of adverse events.
UNCOVER-2: efficacy and adverse events
In UNCOVER-2, 1224 patients were randomly assigned to receive subcutaneous placebo (n=168), etanercept (n=358), or ixekizumab every 2 weeks (Q2W; n=351) or every 4 weeks (Q4W; n=347).
- Participants received subcutaneous placebo, etanercept (50 mg twice weekly), or one injection of 80 mg ixekizumab every two weeks, or every four weeks after a 160 mg starting dose.
- Blinding was maintained with a double-dummy design.
- Co-primary efficacy endpoints were proportions of patients achieving sPGA score 0 or 1 and 75% or greater improvement in PASI at week 12. The analysis was by intention to treat.
- PASI 90, PASI 100, itch numeric rating scale, and Dermatology Life Quality Index (DLQI) were included as secondary endpoints in the study.
- At 12 weeks, the study demonstrated statistically significant superiority of ixekizumab 80 mg Q2W and ixekizumab 80 mg Q4W over placebo.
- The proportion of patients achieving PASI 75 was 89.7% and 77.5% for ixekizumab Q2W and Q4W, respectively, compared to 2.4% in placebo (P < 0.0001 vs placebo).
- The percentage achieving sPGA 0 or 1 was 83.2% and 72.9% for ixekizumab Q2W and Q4W, respectively, compared to 2.4% in placebo (P < 0.0001 vs placebo).
- Both dosage regimens of ixekizumab were statistically superior to placebo in terms of PASI 90, PASI 100, and DLQI (P < 0.0001 vs placebo).
- In comparison to etanercept 50 mg twice weekly, ixekizumab 80 mg Q2W and Q4W were shown to be statistically superior in terms of the proportion of patients reaching PASI 75 and sPGA 0 or 1 at week 12 (P < 0.0001 vs etanercept).
- At 12 weeks, a higher proportion of patients receiving ixekizumab 80 mg Q2W and 80 mg Q4W experienced treatment-related adverse events (61.7% and 58.8%, respectively) compared with placebo.
- The most common adverse events were nasopharyngitis, injection-site reaction, and headache.
- Infections were reported in (29.7% and 28.8%, patients respectively) receiving ixekizumab 80 mg Q2W and 80 mg Q4W compared to placebo (27.5%).
- The proportions of patients with a candida infection at 12 weeks were 1.5% and 0.3% for ixekizumab Q2W and ixekizumab Q4W, respectively, compared to 0.6% for placebo.
- All Candida infections were mild to moderate in intensity and resolved without discontinuation of treatment.
- The rates of serious adverse events at 12 weeks were 1.4%, 2.3%, and 1.2% for patients on ixekizumab Q2W, ixekizumab Q4W, or placebo, respectively.
- At 12 weeks, neutropenia was reported in 8.6% of patients taking ixekizumab Q2W and 7.6% of patients taking ixekizumab Q4W, compared to 4.8% of patients taking a placebo.
- Cases of neutropenia were mild and transient, without associated infections.
- It is important to note that comparisons in adverse events were not statistically significant, as the studies were powered to detect differences in efficacy rather than rates of adverse events.
UNCOVER-3: efficacy and adverse events
Patients in UNCOVER-3 were randomly assigned to receive placebo (n=193), etanercept (n=382), ixekizumab every 2 weeks (Q2W; n=385), or ixekizumab every 4 weeks (Q2W; n=386).
- Primary and secondary efficacy end-points were the same as for UNCOVER-2.
- Like the previous trials, UNCOVER-3 also showed statistically significant superiority of ixekizumab 80 mg Q2W and ixekizumab 80 mg Q4W over placebo.
- The proportion of patients reaching PASI 75 was 87.3% and 84.2% for ixekizumab Q2W and Q4W, respectively, compared to 7.3% in those who took a placebo (P < 0.0001 compared to placebo).
- The percentage achieving sPGA 0 or 1 was 80.5% and 75.4% for ixekizumab Q2W and Q2W, respectively, compared to 6.7% in placebo (P < 0.0001 vs placebo).
- Both ixekizumab regimens were similarly statistically superior to placebo in terms of PASI 90, PASI 100, and DLQI (P < 0.0001 vs placebo).
- As in UNCOVER-2, ixekizumab 80 mg Q2W and Q4W were shown to be statistically superior to etanercept 50 mg twice weekly, in terms of the proportion of patients reaching PASI 75 and sPGA 0 or 1 at week 12 (P < 0.0001 vs etanercept).
- The most common adverse events were nasopharyngitis, injection-site reaction, upper respiratory tract infection, and headache.
- By 12 weeks, a greater proportion of patients receiving ixekizumab 80 mg Q2W and 80 mg Q4W experienced treatment emergent adverse events (53.4% and 56.3%, respectively) or infections (21.4% and 23.0%, respectively), compared to placebo (adverse events: 36.3%, infections: 14.0%).
- The proportions of patients with Candida infection at 12 weeks were 1.8% and 0.8% for ixekizumab Q2W and ixekizumab Q4W, respectively, compared to 0.5% for placebo.
- The rates of serious adverse events at 12 weeks were 2.3, 1.6, and 2.6% for patients on ixekizumab Q2W, ixekizumab Q4W, or placebo, respectively.
- At 12 weeks, neutropenia was reported in 8.9% of patients taking ixekizumab Q2W and 9.5% of patients taking ixekizumab Q4W, compared to 1.0% of patients taking a placebo.
- Cases of neutropenia were mild and transient, without associated infections.
- Comparisons in adverse events are not statistically significant, as the study was powered to detect differences in efficacy rather than adverse events between treatment and placebo.
- A summary of the efficacy results for UNCOVER 1, 2 and three at week 12 are presented in Table 1.
Table 1: Efficacy results at week 12 in evaluable adults with plaque psoriasis in trials 1, 2 and 3
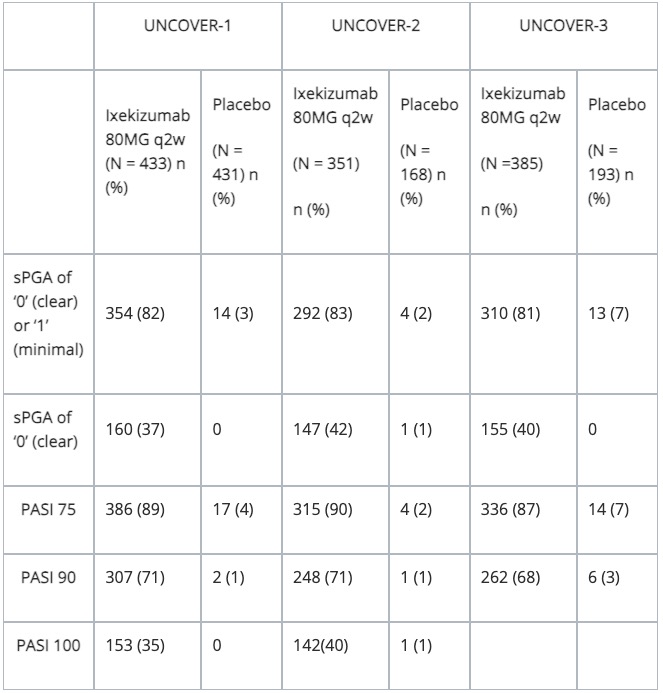
N = number of patients in the intent-to-treat population
Pooled adverse event results in UNCOVER 1, 2 and 3
Adverse events
Table 2 summarises the adverse reactions that occurred at a rate of ≥ 1% in the combined proportion of patients in the Ixekizumab group compared to etanercept and placebo during a 12-week treatment period.
Table 2: Adverse reactions in ≥1% of the TALTZ group vs placebo in adults with plaque psoriasis in trials 1, 2 and 3
Adverse Reactions |
Ixekizumab 80mg Q2W (N = 1167) (n %) |
Etanercept (N = 287) (n %) |
Placebo ( N = 791)(n %) |
Injection site reactions |
196 (17) |
32 (11) |
26 (3) |
Upper respiratory tract infections* |
163 (14) |
23 (8) |
101 (13) |
Nausea |
23 (2) |
1 (1) |
5 (1) |
Tinea infections |
17 (2) |
0 |
1 (1) |
*Upper respiratory tract infections cluster includes nasopharyngitis and rhinovirus infection.
Future directions for ixekizumab
- A large proportion of patients with psoriasis achieve clear or near clear skin during treatment with ixekizumab in a rapid and sustained manner supporting the idea that IL-17A plays a central role in psoriasis immunopathogenesis.
- Ixekizumab 80 mg Q2W and ixekizumab 80 mg Q4W have demonstrated to be more efficacious in terms of PASI 75, PASI 90, and PASI 100 at week 12 compared with etanercept 50 mg twice weekly or placebo. Results are maintained to week 60 and beyond.
- Secukinumab is currently the only other IL-17 pathway inhibitor approved by the US FDA for the treatment of plaque psoriasis.
- Thus far, there have been no head-to-head comparisons of these drugs to directly verify the efficacy and safety of one agent over the other.
- A Phase III clinical trial demonstrated that ixekizumab was statistically superior to placebo in the treatment of patients with active psoriatic arthritis at 24 weeks, as measured by the proportion of patients achieving an American College of Rheumatology 20% improvement response (ACR20).
- Thus ixekizumab may also serve to alleviate the symptoms of psoriatic arthritis and reduce the risk of cardiovascular events associated with elevated levels of IL-17, in patients with psoriasis.
Approved datasheets are the official source of information for medicines, including approved uses, doses, and safety information. Check the individual datasheet in your country for information about medicines.
We suggest you refer to your national drug approval agency such as the Australian Therapeutic Goods Administration (TGA), US Food and Drug Administration (FDA), UK Medicines and Healthcare products regulatory agency (MHRA) / emc, and NZ Medsafe, or a national or state-approved formulary eg, the New Zealand Formulary (NZF) and New Zealand Formulary for Children (NZFC) and the British National Formulary (BNF) and British National Formulary for Children (BNFC).
References
- Gordon KB. Ixekizumab for treatment of moderate-to-severe plaque psoriasis: 60-week results from a double-blind phase 3 induction and randomized withdrawal study (UNCOVER-1). Presented at: 73rd Annual Meeting of the American Academy of Dermatology; San Francisco; 2015 [Abstract F010].
- Griffiths CE, Reich K, Lebwohl M, van de Kerkhof P, Paul C, Menter A, et al Comparison of ixekizumab with etanercept or placebo in moderate-to-severe psoriasis (UNCOVER-2 and UNCOVER-3): results from two phase 3 randomised trials. Lancet. 2015 Aug 8; 386(9993):541–51. PubMed
- Gan EY, Chong WS, Tey HL. Therapeutic strategies in psoriasis patients with psoriatic arthritis: focus on new agents. BioDrugs. 2013 Aug; 27(4):359–73. PubMed
- Armstrong AW, Lynde CW, McBride SR et al. Effect of Ixekizumab Treatment on Work Productivity for Patients With Moderate-to-Severe Plaque Psoriasis: Analysis of Results From 3 Randomized Phase 3 Clinical Trials. JAMA Dermatol. 2016 Mar 7. doi: 10.1001/jamadermatol.2016.0269. [Epub ahead of print]. PubMed
On DermNet
Other websites
- Prescribing information (Ixekizumab, US Label)
- Ixezinumab — European Medicines Agency marketing authorization
- Ixekizumab — Medication Guide. US Label