Acknowledgement
Introduction
Demographics
Causes
Clinical features
Complications
Diagnosis
Assessment
Differential diagnoses
Treatment
Outcome
This document incorporates and summarises information from a number of publications, including guidelines published by the National Institute for Health and Care Excellence (NICE) [1,4], UpToDate [2,7,10,15,16,22,25] and the NZ Formulary [18,19]. It is relevant to the treatment of psoriasis in New Zealand.
In this guideline, psoriasis refers to chronic plaque psoriasis, unless otherwise specified.
Psoriasis is a chronic inflammatory skin disorder that is characterised by disfiguring, scaling and erythematous plaques that may be itchy or painful. Although once thought of as a benign dermatological condition with few serious complications, psoriasis is now considered a multisystem inflammatory disease that is associated with, or increases, the risk of other comorbidities. Psoriasis can be both emotionally and physically debilitating and significantly impact the quality of life [1,2]. [see Psychological effects of psoriasis]
The prevalence of psoriasis worldwide is 0.5% to 11.4% in adults, and 0% to 1.4% in children [3].
Psoriasis is a complex immune-mediated disease. T lymphocytes, dendritic cells, cytokines and tumour necrosis factor are key in the pathogenesis [2].
Chronic plaque psoriasis is the most common type of psoriasis in children and adults, accounting for 55–90% of cases [2,4]. The scalp, extensor elbows, knees and gluteal cleft are the most frequently involved sites. Plaques are erythematous with defined margins and often have a silvery scale. Scale is less evident after bathing or after the application of a moisturiser. The plaques are frequently pruritic. In people with darker skin, hyperpigmentation may be present [2].
Approximately 7–42% of people with psoriasis develop psoriatic arthritis [10].
Comorbidities associated with psoriasis include obesity, metabolic syndrome, cardiovascular disease, malignancy, autoimmune disease (eg, inflammatory bowel disease, coeliac disease and diabetes), chronic kidney disease, non-alcoholic fatty liver disease (NAFLD) [see Liver problems and psoriasis], depression, and alcohol abuse [8,10].
Severe psoriasis can cause death, particularly extensive erythrodermic and pustular psoriasis [2].
Psoriasis is a clinical diagnosis. A skin biopsy can be considered when there is diagnostic uncertainty [2].
Psoriasis is assessed by evaluating:
An objective assessment of psoriasis severity can be made using the static Physician’s Global Assessment (see below) or the Psoriasis Area and Severity Index (PASI). The PASI is generally used in specialist settings [1].
Static Physician’s Global Assessment (sPGA) [13] |
||
|---|---|---|
Induration |
0 - no plaque elevation above the normal skin |
|
Erythema |
0 - no evidence of erythema, hyperpigmentation may be present |
|
Scaling |
0 - no evidence of scale |
|
Average score |
0 = clear, 1 = nearly clear, 2 = mild, 3 = moderate, 4 = severe and 5 = very severe |
|
The patient's assessment of the severity of their psoriasis can be assessed using the static Patient's Global Assessment (graded as clear, nearly clear, mild, moderate, severe or very severe) [1] or a validated self-assessed or patient-oriented PASI score.
Body surface area (BSA) affected can be classified as:
(Note: 0.5% of BSA in adults is approximately equal to the palm of the patient’s hand, excluding fingers [11])
The following features may indicate severe psoriasis due to the impact on the quality of life:
When assessing the impact of psoriasis on physical, psychological and social wellbeing, questions to consider include:
Quality of life measurement is important to properly assess the full effect of an illness such as psoriasis on patients. Two dermatology specific tools to assess the impact on the quality of life are:
People with psoriasis should be screened for psoriatic arthritis annually. This is best achieved in primary care and specialist settings through the use of a validated tool, such as the Psoriasis Epidemiology Screening Tool (PEST) [1]. Consider a non-urgent rheumatology referral or seeking rheumatology advice if the score is > 2 [1,8].
Psoriasis Epidemiology Screening Tool (PEST) [14] |
||
|---|---|---|
Question |
Yes |
No |
Have you ever had a swollen joint (or joints)? |
1 |
0 |
Has a doctor ever told you that you have arthritis? |
1 |
0 |
Do your fingernails or toenails have holes or pits? |
1 |
0 |
Have you had pain in your heel? |
1 |
0 |
Have you had a finger or toe that was completely swollen and painful for no apparent reason? |
1 |
0 |
Consider referral to rheumatology with a score > 2 |
Adults
Assess risk factors and comorbid disease of psoriasis at presentation and as indicated thereafter.
Children
Children with psoriasis [see Paediatric psoriasis] may have higher rates of associated comorbid disease. Recommended screening for risk factors and comorbid disease depend on the child’s age [14].
Eye conditions may occur more commonly in people with psoriasis (blepharitis, conjunctivitis, xerosis, corneal lesions and uveitis). Consider asking patients about ocular symptoms at each follow-up appointment [2].
While psoriasis is treatable, there is no cure [8]. Successful management is dependent on the patient understanding the chronic nature of psoriasis and the therapeutic options that are available to them. Points to consider include:
An acceptable treatment response is either BSA ≤ 3% or an improvement in BSA ≥ 75% from baseline, 3 months after treatment initiation [17].
The ideal target for treatment response is BSA ≤ 1% 3 months after treatment initiation maintained at every 6-month assessment interval during maintenance therapy.
Referral to a dermatologist for advice or face-to-face assessment is recommended in the following circumstances:
Note: Public hospital dermatology services in NZ may have more stringent referral criteria due to a dermatology workforce shortage.
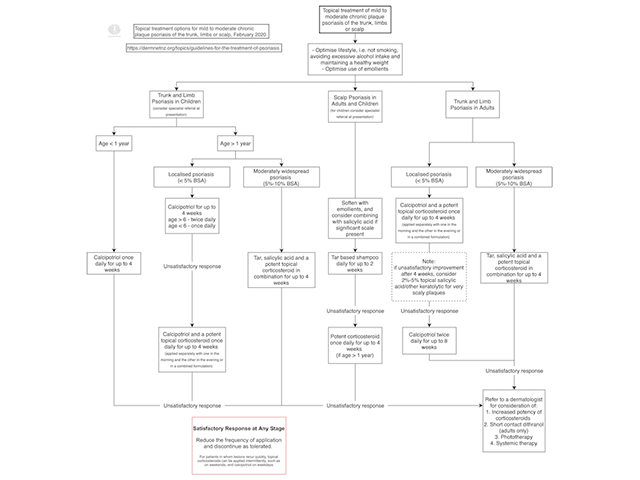
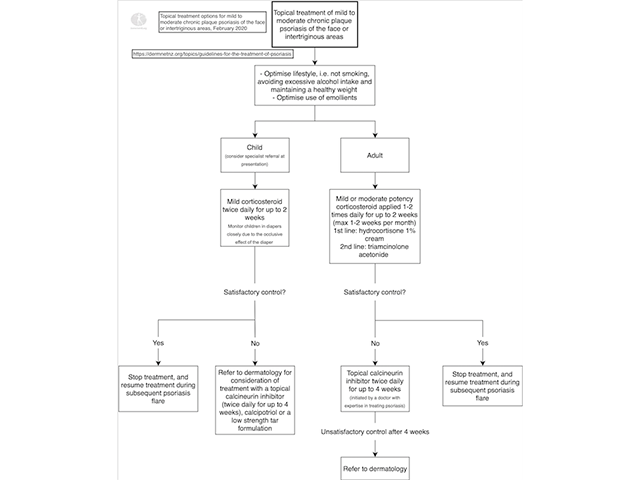
Consider patient preferences, cosmetic and practical aspects of treatment, and the body surface area affected [1].
Moisturiser
Soap substitute
Coal tar
Dithranol
Salicylic acid
Calcipotriol
Corticosteroid
Tacrolimus and pimecrolimus
Tazarotene
Phototherapy appears to slow keratinisation and reduce the activity of T cells implicated in the formation of psoriatic plaques [16].
The following are indications for systemic treatment:
Systemic therapy should be initiated in a specialist setting. Monitoring and supervision can occur in non-specialist settings when these arrangements have been formalised and agreed upon [1].
The NICE guidelines suggest systemic non-biologic therapy should be offered to people with chronic plaque psoriasis if [1]:
Non-biologic systemic therapy outcomes can be optimised with the use of adjunctive topical therapy [1].
All patients using non-biologic systemic therapy need close monitoring for adverse effects, as per local protocols [19,21,23].
Non-biologic systemic agents include methotrexate, ciclosporin, acitretin, and apremilast.
Methotrexate
Ciclosporin
Acitretin
Apremilast
Biologic agents are effective in treating moderate to severe chronic plaque psoriasis. Studies show excellent short and long term results, and treatment is generally well tolerated [16]. While they are often more efficacious than non-biologic systemic therapies, the long term risks are still largely unknown. In addition, biologic systemic therapy is expensive, hence their use in clinical practice remains limited.
In New Zealand, a special authority application is required for a subsidy of biologic treatments [20,21].
Psoriasis often has an unpredictable clinical course. Plaque psoriasis is generally a chronic disease, with fluctuating severity over time. Guttate psoriasis may resolve, relapse, or develop into chronic plaque psoriasis. Generalised pustular psoriasis frequently has a variable and protracted course without intervention [2].
Psoriasis is a multisystem inflammatory disease resulting in an increased risk of mortality compared to those unaffected by psoriasis [2,30]. Specifically, studies suggest an increased liver, kidney, infectious disease and chronic lower respiratory disease mortality risk. Patients with severe psoriasis also appear to have higher cardiovascular disease and neoplasm mortality risk [30]. The cause of the increased mortality risk is unknown. Postulated contributing factors include systemic inflammation, adverse effects of systemic treatments, comorbid conditions and behavioural risk factors [2,30]. Screening and holistic care may help minimise these risks.
Approved datasheets are the official source of information for medicines, including approved uses, doses, and safety information. Check the individual datasheet in your country for information about medicines.
We suggest you refer to your national drug approval agency such as the Australian Therapeutic Goods Administration (TGA), US Food and Drug Administration (FDA), UK Medicines and Healthcare products regulatory agency (MHRA) / emc, and NZ Medsafe, or a national or state-approved formulary eg, the New Zealand Formulary (NZF) and New Zealand Formulary for Children (NZFC) and the British National Formulary (BNF) and British National Formulary for Children (BNFC).

