Introduction Histology Special studies Differential diagnoses
Reticulohistiocytoma (reticulohistiocytosis) is a non-Langerhans cell histiocytosis. Lesions may be solitary (for example solitary cutaneous reticulohistocytoma) or multiple (for example multicentric reticulohistiocytosis). Multicentric reticulohistocytosis is characterized by cutaneous or mucosal papular lesions associated with severe polyarthritis and arthralgias.
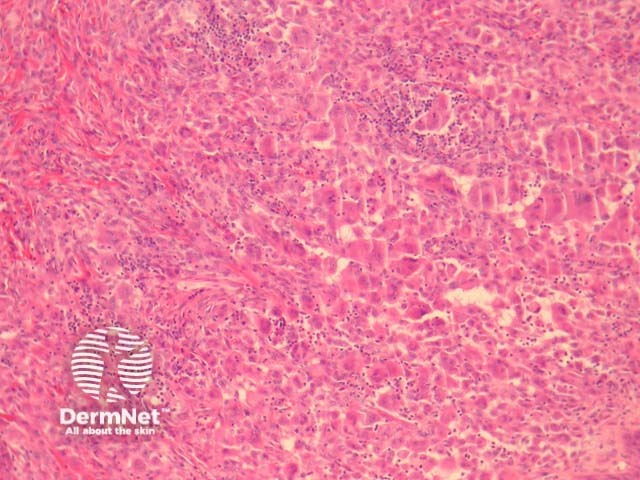
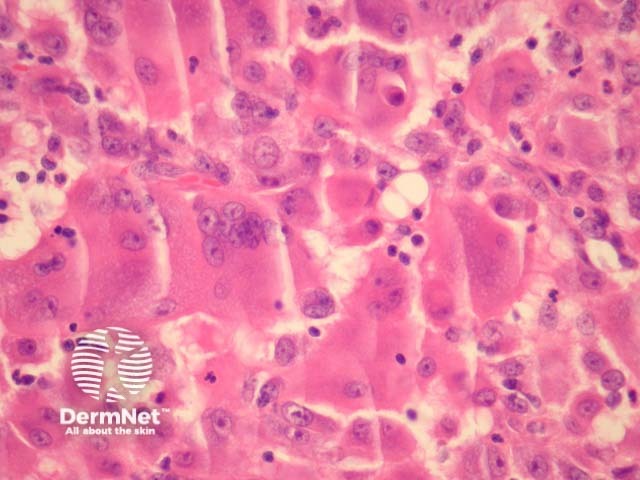
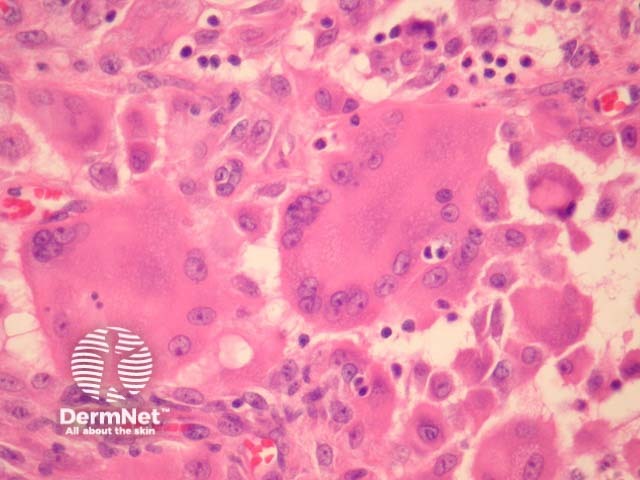
In reticulohistiocytoma, sections show a diffuse infiltration of numerous large, mononucleated or multinucleated histiocytes in the dermis (figures 1-3). There are associated lymphocytes and dermal fibrosis. Characteristically, the lesional cells have a dense pink cytoplasm, variously referred to as “oncocytic” or “ground glass” (figures 2, 3).
Reticulohistiocytoma cells are positive with CD68 and Factor 13a. S100 and CD1a are typically negative.
Other histiocytic diseases: these typically lack the characteristic “ground glass” cytoplasm seen in reticulohistiocytoma. In addition to morphologic features, CD1a and S100 immunohistochemical studies can be used to exclude Langerhans cell histiocytosis and Rosai-Dorfman disease respectively.
Juvenile xanthogranuloma shows “Touton” giant cells, and lipidisation of histiocytes. The rarer histocytoses may require more extensive immunohistochemical studies and clinical correlation.

