

Rosai-Dorfman disease pathology — extra information
Introduction Histology Special studies Differential diagnoses
Introduction
Rosai-Dorfman Disease, also called sinus histiocytosis with massive lymphadenopathy, is a non-Langerhans histiocytic disease. The skin is the most common extranodal site. Cutaneous Rosai-Dorfman disease typically occurs in older females and presents in various forms, ranging from single papules to multiple nodules and plaques.
Histology of Rosai-Dorfman disease
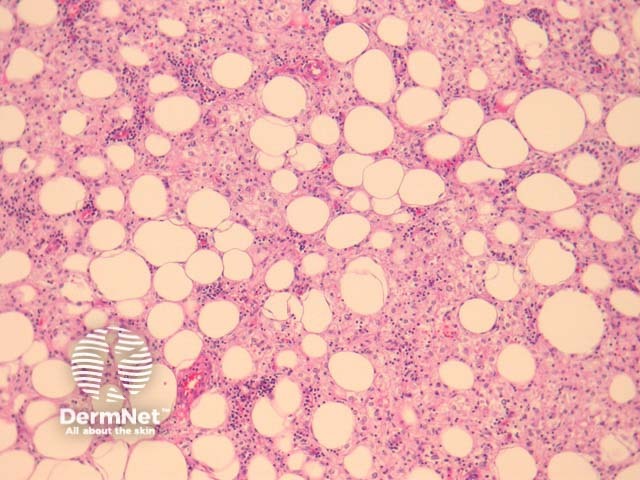
Rosai-Dorfman shows infiltration of the dermis or subcutaneous tissue with associated sclerosis (figures 1, 2). The infiltrate is composed predominantly of epithelioid histiocytes with a pale to eosinophilic cytoplasm. Some multinucleate forms may be seen. Admixed with these large histiocytes are lymphocytes, plasma cells, neutrophils and eosinophils.
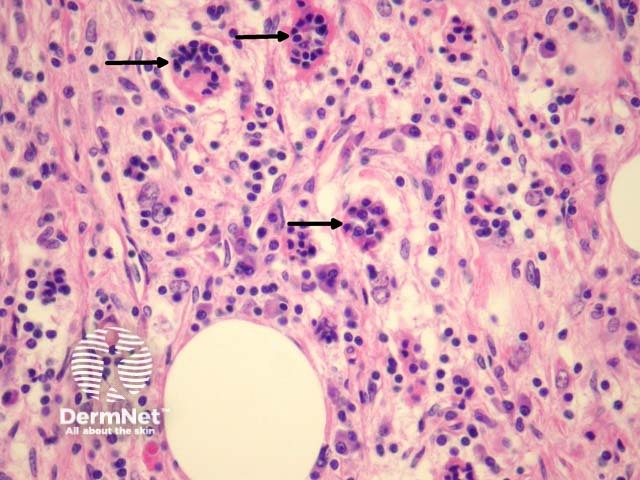
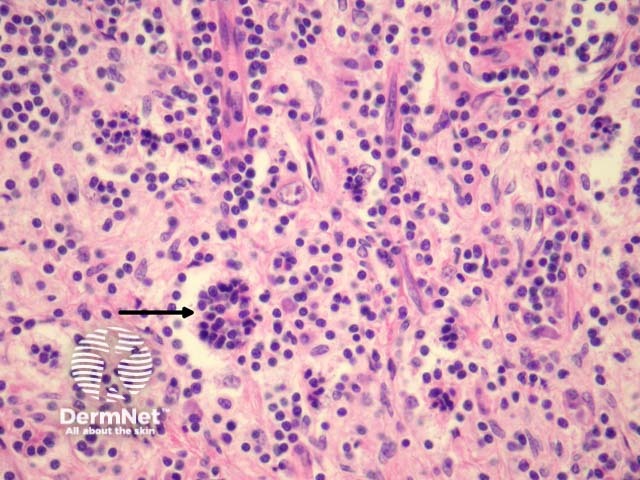
The hallmark of Rosai-Dorfman disease is emperipolesis, in which lymphocytes and other inflammatory cells reside undisturbed within the cytoplasm of the histiocytes (figures 3, 4, arrows).
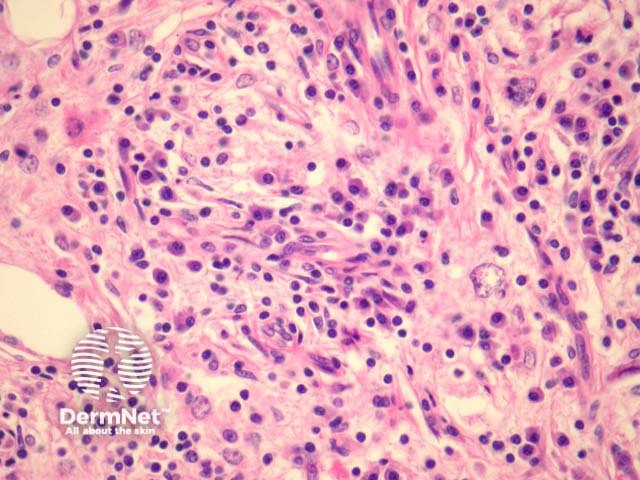
Plasma cells are frequently dense in cutaneous Rosai-Dorfman disease (figure 5). Because of this, some authors believe there is a relationship this disease and IgG4-related sclerosing diseases.

Special studies for Rosai-Dorfman disease
Histiocytes show positive staining for CD68 and S-100 in Rosai-Dorfman disease. CD1A is negative.
Differential diagnosis of Rosai-Dorfman disease
Other histiocytic diseases should not display emperipolesis.
- Langerhans cell histiocytosis: CD1a and S100 immunohistochemical studies can be used to exclude.
- Reticulohistiocytoma: characteristic “ground glass” cytoplasm.
- Juvenile xanthogranuloma: “Touton” giant cells, and lipidisation of histiocytes. The rarer histocytoses may require more extensive immunohistochemical studies and clinical correlation.
Subcutaneous panniculitis-like T-cell lymphoma: the infiltrate is predominantly lymphocytic. There are histiocytes engulphing nuclear debris (bean bag cells) which should not be confused with emperipolesis. The lymphocytes demonstrate nuclear atypia and can be seen to characteristically rim the adipocytes.
References
- Brenn T, Calonje E, Granter SR, Leonard N, Grayson W, Fletcher CDM, et al. Cutaneous Rosai-Dorfman disease is a distinct clinical entity. Am J Dermatopathol. 2002;24:385–91. PubMed
- Kuo TT, Chen TC, Lee LY, Lu PH. IgG4-positive plasma cells in cutaneous Rosai-Dorfman disease: an additional immunohistochemical feature and possible relationship to IgG4-related sclerosing disease. J Cutan Pathol. 2009 Oct;36(10):1069–73. PubMed
On DermNet