Trichophyton mentagrophytes genotype VII (TMVII) is a rare dermatophyte strain that causes an inflammatory and persistent superficial fungal infection, typically of the anogenital and facial skin. It is known to spread between humans during intimate or sexual skin-to-skin contact.
TMVII infection can resemble acute viral and bacterial infections, which can delay diagnosis.
TMVII infection predominantly occurs in men who have sex with men (MSM), with heterosexual transmission being reported less frequently.
Other risk factors include:
Sexual transmission of Trichophyton mentagrophytes genotype VII has been recognised since 2002.
Trichophyton mentagrophytes genotype VII is an anthropophilic (human host) variant of Trichophyton mentagrophytes, a largely zoophilic (animal host) dermatophyte species.
The primary mode of transmission is direct skin-to-skin contact with an infected individual, including sexual contact. Cases of transmission from massage treatments have also been reported.
Dermatophytosis caused by Trichophyton mentagrophytes genotype VII can present as tinea cruris, tinea genitalis/pubogenitalis, tinea faciei, tinea barbae, and tinea corporis. The incubation period for lesions to appear is approximately 10 to 18 days.
Lesion features:
In hair-bearing areas, particularly the face, there may be hair loss.


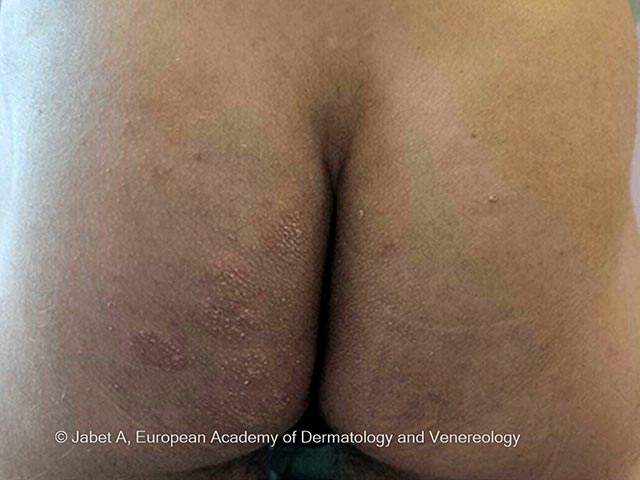

Early erythema may be less evident in darker skin types.
A diagnosis of tinea can be made with microscopy or fungal culture. However, DNA sequencing is required to confirm TMVII and distinguish it from related species such as T. interdigitale or T. mentagrophytes genotype VIII.
Oral agents should be used for at least 4 weeks, or until lesions have resolved or the individual is mycologically negative. Similar dermatophyte species have shown resistance to both of these oral agents, though this has not yet been observed in TMVII.
Avoid direct skin-to-skin contact or sharing personal items (eg, towels, bedding, clothing) with infected individuals.
Cure is expected with appropriate oral antifungal treatment. Untreated, the infection can disseminate widely over the skin, and there is the potential for scarring and permanent hair loss. Reinfection from another infected individual is possible.

