Introduction - vaginitis Introduction Demographics Cause Clinical features Complications Diagnosis Differential diagnoses Treatment
The term 'vaginitis' means an inflamed vagina; the term is loosely used to refer to any vaginal condition that results in a vaginal discharge, whether due to infectious or non-infectious causes.
Aerobic vaginitis is characterised by:
Aerobic vaginitis was first characterised by Donders et al in 2002. Desquamative inflammatory vaginitis is a severe form of aerobic vaginitis [1,2].
Aerobic vaginitis may affect adult women of any age, whether pre- or post-menopause. The prevalence of aerobic vaginitis has been estimated in different populations as being present in 5–13% of asymptomatic women and affecting a greater proportion of women with vaginal symptoms. It may be less prevalent among pregnant women.
The risk factors for infection are under evaluation.
The cause of aerobic vaginitis is unknown. Aerobic vaginitis is a form of dysbiosis, a disturbance in the ecology of aerobic micro-organisms that reside in the vaginal microflora (the microbiome). These microorganisms include:
It is unclear whether the primary cause of aerobic vaginitis is pathogenic organisms, lack of lactobacilli, immune dysregulation and pro-inflammatory cytokines, or insufficient oestrogen in the vaginal mucosa (atrophic vulvovaginitis) [2].
The symptoms of aerobic vaginitis can fluctuate over a long period of time. They include [2]:
Examination findings may include:
Aerobic vaginitis has been associated with [2]:
The diagnosis of aerobic vaginitis is confirmed by wet–mount microscopy of fresh vaginal fluid, ideally using phase contrast. The aerobic vaginitis score is graded as 0–3 (absent), 3–4 (mild), 5–6 (moderate), and 6–10 (severe). The aerobic vaginitis score is calculated from the [1]:
Vaginal cultures are useful only for clinical research and to detect group A streptococci, trichomoniasis, and Candida albicans infection.
Various advanced diagnostic methods are being established for aerobic vaginitis.
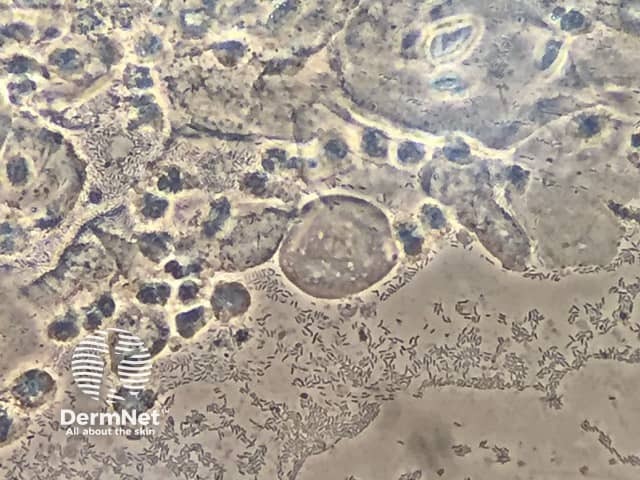
*Credit: Pedro Vieira Baptista
Aerobic vaginitis is distinct from other forms of infectious vaginitis — particularly bacterial vaginosis, with which it is often confused. The characteristics of bacterial vaginosis are:
The treatment of aerobic vaginitis depends on the microscopic findings and patient needs [2].
Metronidazole, which is used for bacterial vaginosis, and antifungal agents, used for Candida albicans infection, are not effective in aerobic vaginitis.
Expert advice should be sought from a medical microbiologist in pregnant women with aerobic vaginitis.

