Introduction
Demographics
Causes
Clinical features
Variation in skin types
Complications
Diagnosis
Differential diagnoses
Treatment
Prevention
Outcome
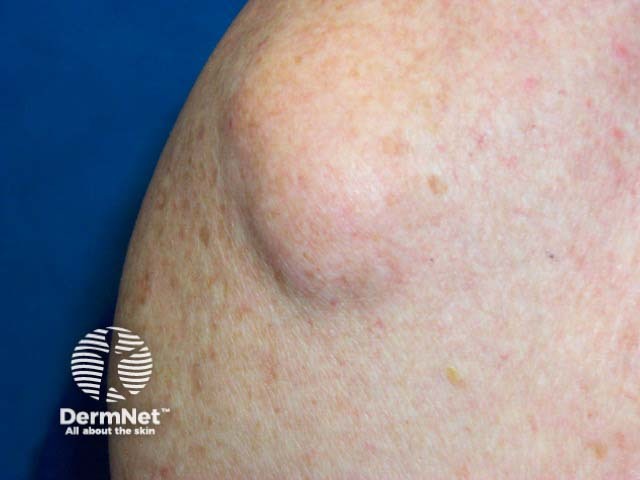
Dercum disease is a rare condition characterised by the gradual and progressive development of benign painful subcutaneous lipomas and angiolipomas that vary in size, number, and location.
It was first described in 1892, by Dercum, who named the disease 'adiposis dolorosa' to describe the painful adiposities (fat accumulations) seen in his 3 patients. It is also known as adiposalgia and Ander syndrome.
The condition causes significant morbidity due to chronic, often treatment-resistant pain, which greatly impairs the quality of life for those affected.

Dercum disease is deemed a rare disorder by The National Organisation for Rare Disorders (NORD; eg, affects less than 200,000 individuals in the United States). The exact prevalence is unknown due to the limited number of reported cases.
Although it was initially thought to predominantly affect post-menopausal women, recent studies have challenged this view, and this is no longer widely accepted.
The pathogenesis is not well-understood. Several theories have been proposed to explain the development of the disease, including an underlying defect in lipid metabolism, trauma-induced lesions, mechanical pressure from growing adipose deposits on nerves, or dysregulation of the autonomic nervous system.
Dercum disease is mostly sporadic, though some case reports describe familial occurrences, inherited in an autosomal dominant pattern with incomplete penetrance. No specific genes have been implicated in its development. Establishing the hereditary nature of Dercum's disease has been challenging, largely due to difficulties in distinguishing it from other similar conditions, such as Madelung syndrome (benign symmetric lipomatosis) and familial multiple lipomatosis.
Dercum disease has several cardinal features, including:
Other features that may be associated include chronic fatigue, weakness, and neuropsychiatric disturbances such as depression, anxiety, migraines, cognitive difficulties, memory impairment, and sleep disturbances. Additionally, fibromyalgia is commonly seen as a comorbidity in those affected by the condition.
Several classification systems have been proposed for Dercum disease over time. However, the currently accepted system divides the disease into four subtypes, based on variations in pain and the localisation of adipose deposits.
Classification |
Description |
Dercum disease Type I |
A generalised diffuse form with widespread painful adipose tissue without distinct lipomas |
Dercum disease Type II |
A generalised nodular form with diffuse pain in the adipose tissue accompanied by intense pain in and around multiple lipomas |
Dercum disease Type III |
A localised nodular form with pain in and around multiple lipomas |
Dercum disease Type IV |
A juxta-articular form with painful lipomas in the periarticular soft tissue |
Dercum disease does not appear to be influenced by Fitzpatrick skin types or race.
Dercum disease may lead to:
Dercum disease is diagnosed through a detailed patient history and physical examination, as there are no specific diagnostic tests or validated criteria available. It is important to rule out other causes of multiple lipomas.
The following investigations may be considered:
Blood:
Tissue biopsy:
Imaging:
Dercum disease must be differentiated from the following diseases:
Madelung disease (multiple symmetric lipomatosis)
Familial multiple lipomatosis
Fibromyalgia
Other differential diagnoses include:
Dercum disease is associated with severe, chronic pain that is challenging to treat. Some degree of trial and error is often required to individualise therapies to provide adequate symptomatic relief for each patient; chronic pain specialists may be required. The overall goal of treatment is to relieve symptoms and improve quality of life.
Some of the interventions below may be combined to achieve the best possible outcome.
Localised interventions:
Systemic pharmacological interventions:
Surgical interventions:
Dercum disease may be prevented by promoting and maintaining a healthy lifestyle to prevent obesity.
Dercum disease runs a chronic course and long-term follow up is often necessary. The disease activity may fluctuate requiring extended therapy ranging from months to years.
The response to treatment is also often unpredictable and while short-term relief may be achieved, the recurrence of pain is common, contributing to the high morbidity associated with this disease.
If left untreated and without good support, prognosis is less favourable leading to increasingly debilitating physical and mental health consequences.

