

Dermoscopy of benign melanocytic lesions
Created 2008.
Learning objectives
- Describe dermatoscopic features of benign melanocytic lesions
Introduction
Benign pigmented skin lesions may be melanocytic or non-melanocytic in origin. Specific dermatoscopic features suggesting melanocytic origin include the presence of:
- Pigment network
- Aggregated brown or black globules
- Specific features: parallel pattern on palms and soles, follicular openings on facial skin, homogeneous steel-blue of blue naevus.
Most individuals have a predominant type of naevus. There is some variation according to age.
Acquired naevi
Global structure
Benign melanocytic lesions have a well-organised structure, tending to be symmetrical and with uniform structure. They may be flat, flat peripherally and raised centrally, or entirely elevated.
Benign melanocytic naevi


Elevated naevi may have a positive ‘wobble sign’ (they can be shifted using the dermatoscope).



Dermoscopy may show melanocytic naevi to be composed entirely of:
- Cobblestone pattern (dermal naevi)
- Aggregated globules
- Pigment network (reticular pattern)
- Homogeneous/amorphous (structureless) pigmentation
The cobblestone pattern are the predominant pattern of congenital naevi. Aggregated globules are the predominant pattern of childhood naevi. A network arises in adolescents and adults presumably provoked by sun exposure. These naevi may become homogeneous in time.
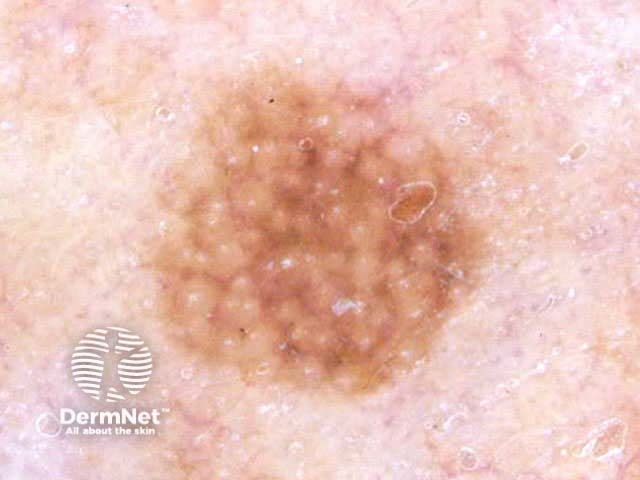
Benign melanocytic naevi: structural patterns




A pointillist naevus is composed of multiple tiny brown or black dots on dermoscopy. It is uncommon.
Pointillist naevus


The blue naevus is a uniform steel blue colour on dermoscopy. A cellular blue naevus, found on the buttocks, has pale or yellowish areas on the periphery and can resemble dermatofibroma. A combined naevus consists of a blue naevus in combination with a congenital, common, atypical or Spitz naevus.
Blue naevus




Colours
The colour of the lesion may be black (especially in dark skinned individuals), brown (junctional naevus), skin coloured or pink (cellular or dermal naevus), steel-blue (blue naevus). Lesions of a single colour or uniform pigment pattern are nearly always benign. Darker skinned individuals tend to have darker naevi.
Benign melanocytic naevi: colours



Two or more colours may be seen in benign lesions, usually symmetrically distributed, for example a network pattern surrounding a central amorphous area, or a regular pattern of dark and light areas.
Benign melanocytic naevi: two colours



Vascularity
The vascular pattern of a benign melanocytic naevus is often difficult to see. However, a uniform pattern of prominent blood vessels is often visible in skin coloured or pink dermal naevi; these may have hair pin appearance. The vessels are most often comma-like/peripheral but can be hairpin or arborising, which may result in confusion with basal cell carcinoma.
Benign melanocytic naevi: uniform vasculature




Border
Most melanocytic naevi have a border that gradually fades out with paler colour on the periphery. However there may be a sharp border in the following benign lesions:
- Ephelis: moth-eaten edge
- Blue naevus: steel-blue uniform pigmentation
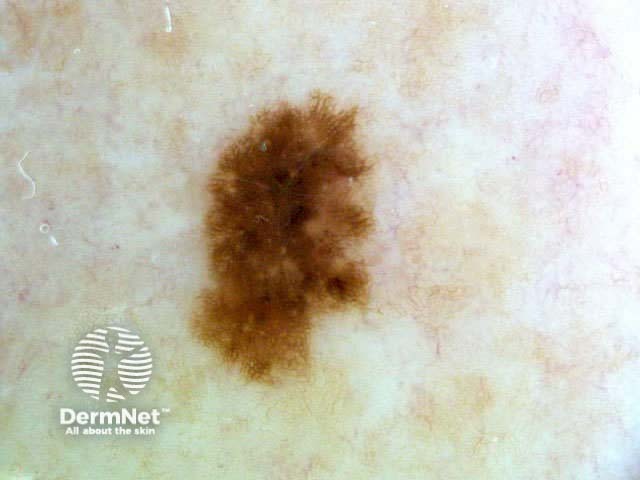
- Pigmented Spitz naevus: peripheral globules are also often seen around a structureless centre
- Reed naevus: ‘starburst’ pattern, circumferential radial streaming
- Globular pattern of benign naevus
Benign melanocytic naevi: sharp border





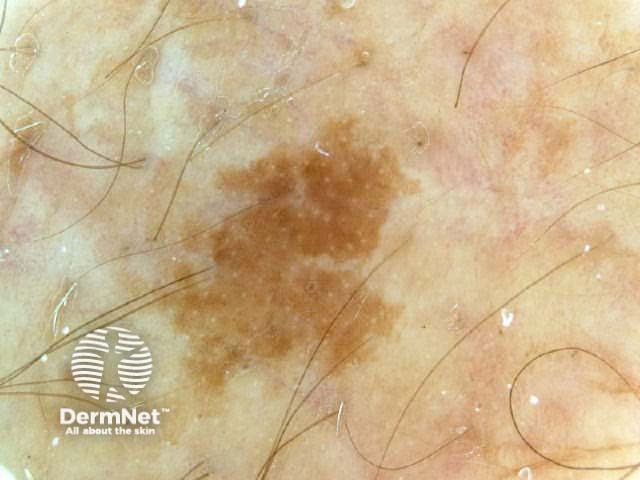
Freckles
Flat melanocytic lesions or freckles include ephelis, solar lentigo and lentigo simplex. These are distinguished by their histological features.
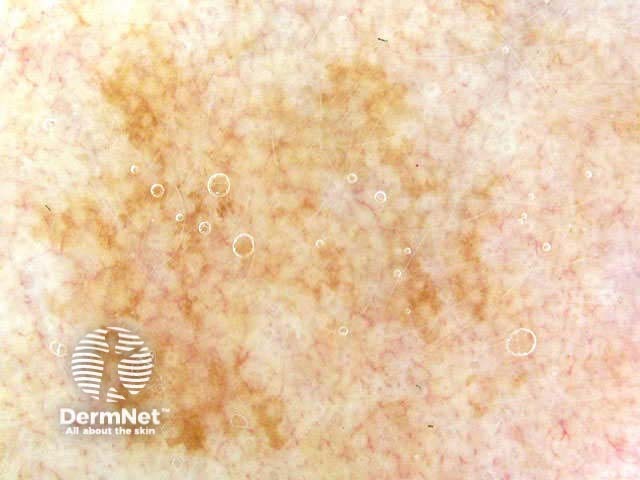
Ephelis
The ephelis is a solar-induced macule with a normal number of melanocytes that produce increased melanin, which is distributed among keratinocytes. Dermoscopy of an ephelis generally shows uniform pigmentation and a moth-eaten edge.



Lentigo simplex
The lentigo simplex has increased melanocytes producing increased melanin. Dermoscopy characteristically shows a dark uniform network across the whole lesion. Very dark lesions are known as ink spot lentigos. Blue pigmentation occurs in some lesions due to dermal melanophages.




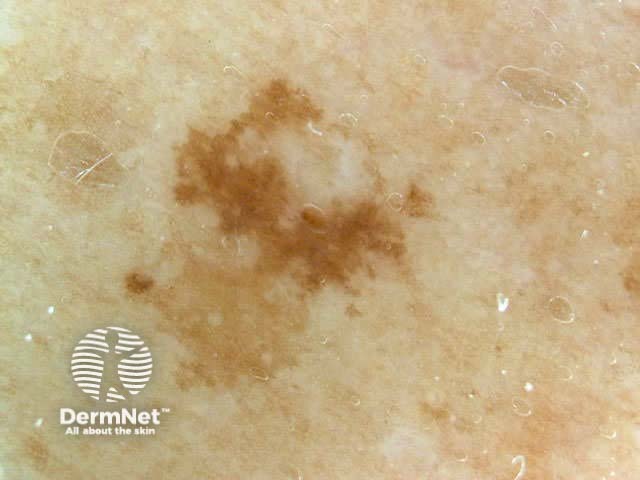
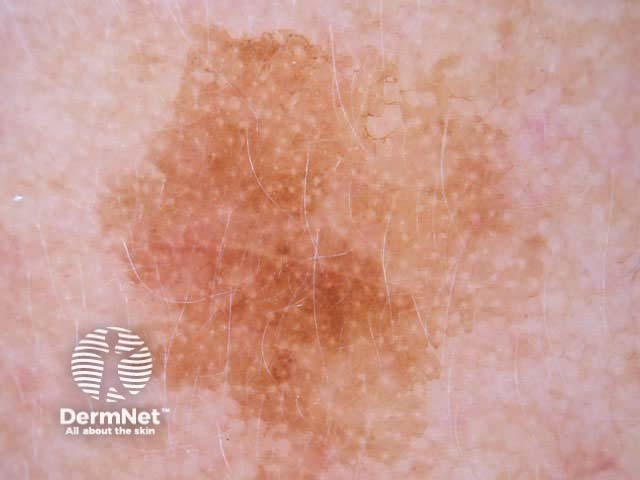
Solar lentigo
The solar lentigo is a solar-induced macule with solar elastosis, elongated rete ridges and a normal number of melanocytes producing increased melanin. They may evolve into seborrhoeic keratosis. Dermoscopy of a solar lentigo may show a faint pigmented network or fingerprint structures or uniform pigmentation.


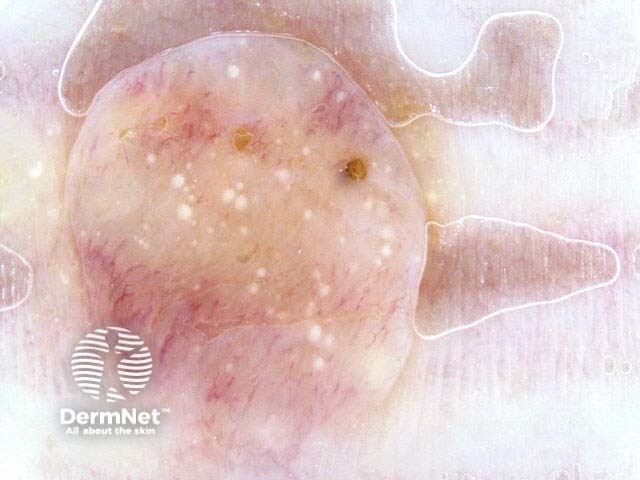
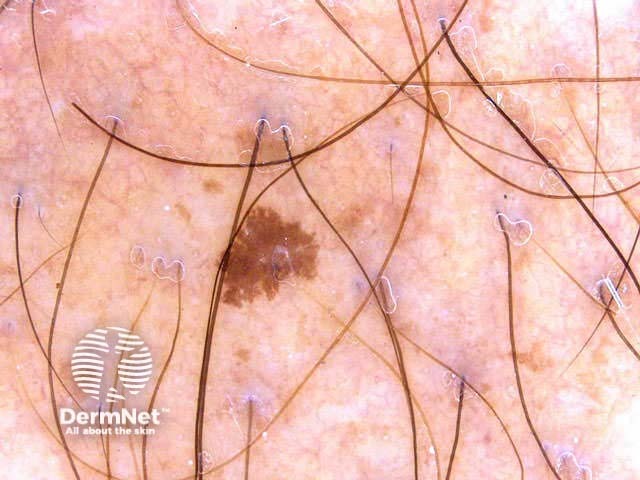
Congenital melanocytic naevi
Congenital melanocytic naevi may be recognised dermatoscopically by the following features:
- Frequently, large size and asymmetrical shape
- Terminal hairs
- Cobblestone/globular or homogenous pattern or multicomponent pattern
- Black or brown dots and globules
- Milia-like cysts
- Crypts and fissures
- Up to 4 colours (uniformly scattered, central hypopigmentation or central hyperpigmentation)
- Congenital Melanocytic Naevi often have prominent symmetric hypopigmented areas.
The presence of asymmetry, multiple colours, and multicomponent pattern on dermoscopy may give rise to concern that a lesion is melanoma. A history of change within the lesion should be taken seriously as melanoma may arise in congenital melanocytic naevi, especially in giant naevi.
At times it can be difficult to distinguish seborrhoeic keratoses from congenital melanocytic naevi that have milia-like cysts, crypts and fissures. Naevi tend to have a more uniform structure than seborrhoeic keratoses.




Special sites
Mucosal melanosis
Benign melanosis of mucosal surfaces (lips, vulva, penis) is relatively featureless on dermoscopy showing uniform amorphous pigmentation.




Palms and soles
Pigment distribution within the furrows is typical on palms and soles. Sometimes the pigmentation in these lesions is described as parallel, fibrillar or filamentous, lattice-type or homogenous. Globules are occasionally seen.
The parallel furrow pattern most often appears in naevi on the side of the foot. The fibrillar pattern appears more likely in lesions on weight bearing sites, and the lattice pattern on the arch of the foot.




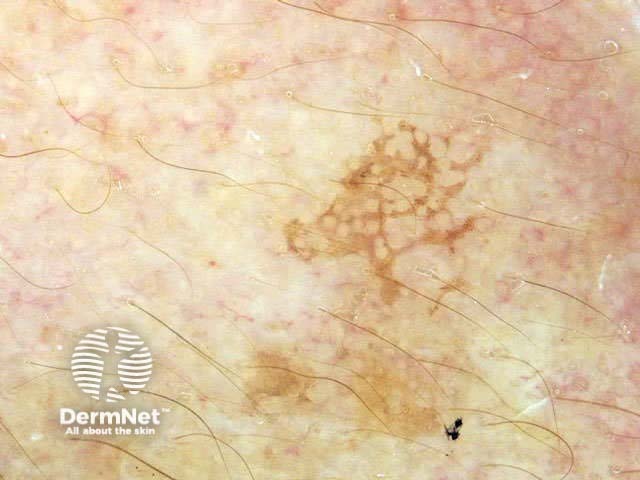
Facial lesions
Melanocytic and non-melanocytic lesions on the face are often characterised by a pseudonetwork, with a broad annular pattern of pigmentation around numerous and prominent hair follicles. The pseudonetwork in benign lesions is symmetrical and regular. Some solar lentigines do not have pseudonetwork and are uniformly amorphous; the flat seborrhoeic keratosis with dry or scaly surface may reveal white reflected or dull yellow keratin.

Nails
Benign naevi may result in one or more parallel longitudinal bands of pigment on the nail plate. On dermoscopy, the colour is uniform and equal in diameter at the proximal and distal ends of the band, which may arise within a pale brown background. Naevi may be congenital, in which case there may be some variation in thickness and colour of the pigmented bands. A uniformly pale brown nail may be a lentigo.
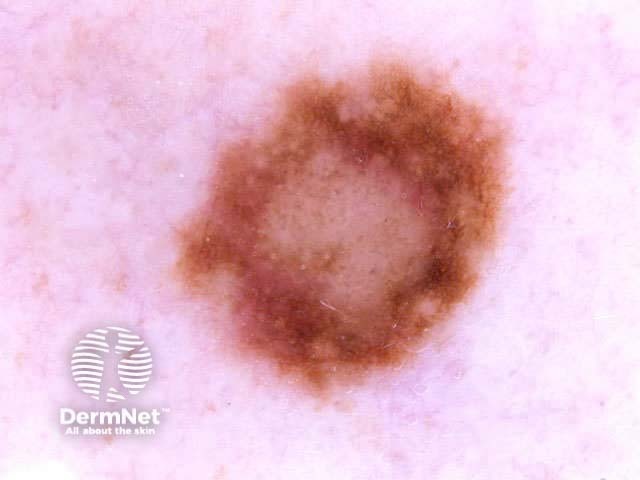
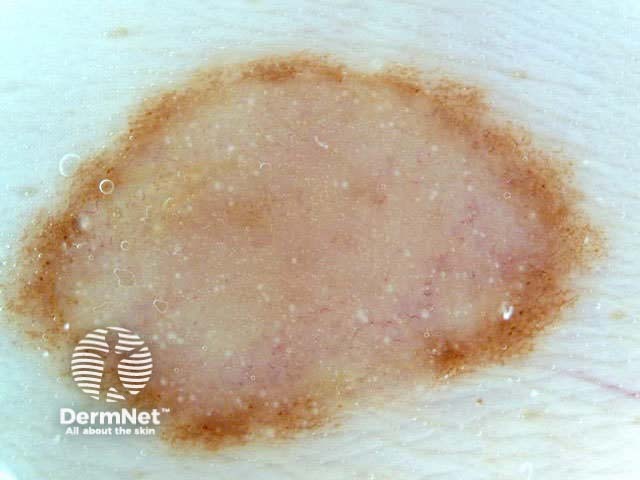
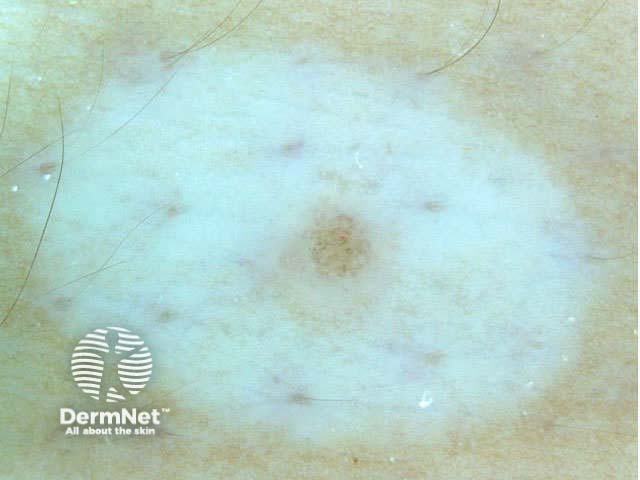
Halo naevi
Halo naevi fade away because of an immune reaction. Clinically the mole is surrounded by hypopigmentation or achromia. Dermoscopy shows symmetrical peripheral hypopigmentation without scarring. The central naevus may be typical or atypical, fully developed or fading away. Globular and homogeneous patterns may be seen. Evolving halo naevi may be observed by dermoscopic monitoring to slowly disappear over months to several years.
The pseudohalo naevus is a normal mole that has been protected from sun exposure, e.g., with sunscreen or a plaster, preventing tanning of the skin adjacent to the lesion. The mole in the middle is of normal structure and does not evolve.



Activity
Examine numerous melanocytic lesions. Train yourself to recognise normal dermoscopic features.
Page 5 of 18. Next topic: Dermoscopy of atypical naevi. Back to: Dermoscopy contents.
New topic – Melanocytic naevi: new classification
References
- Carli P, De Giorgi V, Massi D, Giannotti B. The role of pattern analysis and the ABCD rule of dermoscopy in the detection of histological atypia in melanocytic naevi. Br J Dermatol. 2000 Aug;143(2):290-7. Medline.
- Oliveria SA, Geller AC, Dusza SW, Marghoob AA, Sachs D, Weinstock MA, Buckminster M, Halpern AC. The Framingham school nevus study: a pilot study. Arch Dermatol. 2005 May;140(5):545-51. Medline.
- Zalaudek I, Grinschgl S, Argenziano G, Marghoob AA, Blum A, Richtig E, Wolf IH, Fink-Puches R, Kerl H, Soyer HP, Hofmann-Wellenhof R. Related Articles, Links Abstract Age-related prevalence of dermoscopy patterns in acquired melanocytic naevi. Br J Dermatol. 2006 Feb;154(2):299-304. Medline.
On DermNet
- Moles
- Dermatoscope overview
- Dermatoscopy quizzes
- Dermatoscopy Information for patients
- Image acquisition
Books about skin diseases
See the DermNet bookstore