Introduction
Demographics
Causes
Clinical features
Complications
Diagnosis
Treatment
Outlook
Lichen sclerosus is a common chronic inflammatory skin disorder that most often affects genital and perianal areas.
Older names for lichen sclerosus include lichen sclerosus et atrophicus, kraurosis vulvae (in women), and balanitis xerotica obliterans (in males).


Lichen sclerosus can start at any age, although it is most often diagnosed in women over 50. Pre-pubertal children can also be affected.
The cause of lichen sclerosus is not fully understood and may include genetic, hormonal, irritant, traumatic, and infectious components.
Lichen sclerosus is often classified as an autoimmune disease. Autoimmune diseases are associated with antibodies to a specific protein.
Male genital lichen sclerosus is rare in men circumcised in infancy. It has been suggested that it may be caused by chronic, intermittent damage by urine occluded under the foreskin.
As onset in women is commonly postmenopausal, a relative lack of oestrogen may be significant.
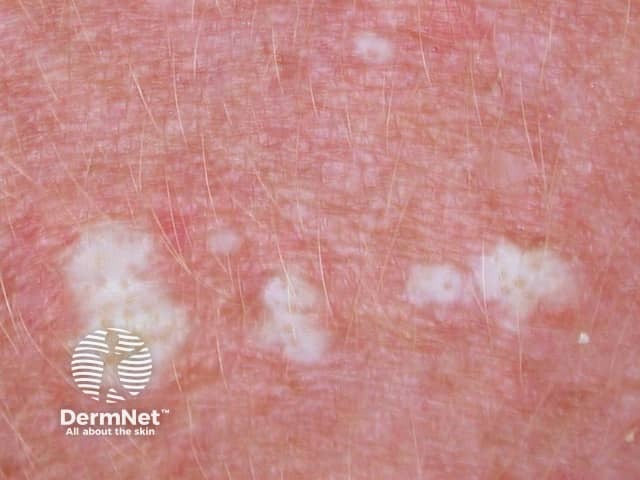
Lichen sclerosus presents as white crinkled or thickened patches of skin that tend to scar.
Lichen sclerosus primarily involves the non-hair bearing, inner areas of the vulva.
Lichen sclerosus can be extremely itchy and sore (see Pruritus vulvae).
Lichen sclerosus causes adhesions and scarring.
See Vulval lichen sclerosus images.
See Perianal lichen sclerosus images.
See Anogenital lichen sclerosus in skin of colour images.
In men, lichen sclerosus usually affects the tip of the penis (glans), which becomes white, firm and scarred. [see Lichen sclerosus in men]
See Images of penile lichen sclerosus.
See Anogenital lichen sclerosus in skin of colour images.
Extragenital lichen sclerosus refers to lichen sclerosus at other sites.
One or more white dry plaques may be found on the inner thigh, buttocks, lower back, abdomen, under the breasts, neck, shoulders, and armpits.



See more on Extragenital lichen sclerosus images.
Patients with lichen sclerosus may develop infections, particularly Candida albicans, herpes simplex, Staphylococcus aureus. Herpes infections are particularly painful and may cause vulval ulceration.
Lichen sclerosus of anogenital sites is associated with an increased risk of vulval, penile or anal cancer (squamous cell carcinoma, SCC).
Extragenital lichen sclerosus does not appear to predispose to cancer.
An experienced clinician can often diagnose lichen sclerosus by its appearance. Dermoscopy can provide further clues. Skin biopsy is frequently recommended.
A biopsy may also be recommended at follow-up, to evaluate areas of concern or to explain the inadequate response to treatment.
Patients with lichen sclerosus are best to consult a doctor with a particular interest in the condition for accurate diagnosis and treatment recommendations.
They are advised to become familiar with the location and appearance of their lichen sclerosus.
Topical steroids are the primary treatment for lichen sclerosus. An ultrapotent topical steroid is often prescribed (eg, clobetasol propionate 0.05%). A potent topical steroid (eg, mometasone furoate 0.1% ointment) may also be used in mild disease or when symptoms are controlled.
The doctor should reassess the treated area after a few weeks, as a response to treatment is quite variable.
Topical steroids are safe when used appropriately. However, excessive use or application to the wrong site can result in adverse effects. In anogenital areas, these include:
It is most important to follow instructions carefully and to attend follow-up appointments regularly.
Other topical treatments used in patients with lichen sclerosus include:
When lichen sclerosus is severe, acute, and not responding to topical therapy, systemic treatment may rarely be prescribed. Options include:
Surgery is essential for high-grade squamous intraepithelial lesions or cancer.
In males, circumcision is effective in lichen sclerosus affecting prepuce and glans of the penis. It is best done early if initial topical steroids have not controlled symptoms and signs. If the urethra is stenosed or scarred, reconstructive surgery may be necessary.
In females, the release of vulval and vaginal adhesions and scarring from vulval lichen sclerosus may occasionally be performed to reduce urination difficulties and allow intercourse if dilators have not proved effective. Procedures include:
Unfortunately, lichen sclerosus sometimes closes up the vaginal opening again after surgery has initially appeared successful. It can be repeated.
Other reported treatments for lichen sclerosus are considered experimental at this time.
Lichen sclerosus is a chronic disease and usually persists for years.
Long-term follow-up is recommended to monitor the disease, optimise treatment and ensure early diagnosis of cancer.

