Introduction
Demographics
Causes
Clinical features
Complications
Diagnosis
Differential diagnoses
Treatment
Outcome
Hyperkeratosis lenticularis perstans (HLP), also known as Flegel disease, is a rare heritable disorder of keratinisation that was first described by Flegel in 1958. It is characterised by red-brown papules with irregular horny scales located mainly on the dorsal aspect of the feet and lower legs. It has been regarded as a variant of Kyrle disease, however its clinical and pathological features are sufficiently distinct to establish it as a separate disease entity.





This condition:
Hyperkeratosis lenticularis perstans is an autosomal-dominant genodermatosis, although sporadic cases are commonly reported.
The underlying cause of this disease is due to heterozygous pathogenic variants in the SPTLC1 gene, which encodes serine palmitoytransferase (SPT), specifically the long chain base subunit -1 (SPTLC1). SPTLC1 is the key enzyme in sphingolipid biosynthesis.
Frameshift or splicing variants in this gene lead to nonsense-mediated mRNA decay, hence reducing SPTLC1 protein levels. This reduction leads to the development of HLP.
As for the sporadic cases, there is no clear understanding of the specific triggers for HLP. It has been associated with several systemic conditions, including adult-onset diabetes, hyperaldosteronism, and hyperthyroidism.
Lesions are small, red-brown, 1–5 mm scaly papules distributed symmetrically on the dorsal aspect of the feet and lower legs. Removal of the scale reveals a bright red base, often with pinpoint bleeding. The papules are asymptomatic, except for rare episodes of mild pruritus or burning sensation.
Less typical sites of occurrence have been reported such as axillae, eyes, palms and soles, single leg involvement, trunk, upper extremities, buttocks, forehead, outer ear lobes, and oral mucosa.
HLP is asymptomatic and has no serious complications. Hence, it is considered mostly an aesthetic issue.
Hyperkeratosis lenticularis perstans can usually be diagnosed clinically, especially if there is a family history of HLP, and confirmed on a skin biopsy with histological features of focal compact hyperkeratosis, thinned stratum Malpighii, epidermal atrophy, and a dense, band-like lymphocytic infiltrate in the papillary dermis.
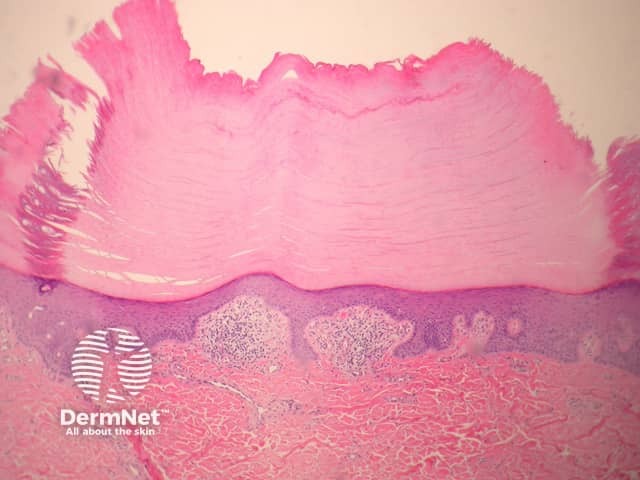
The histopathology of HLP - marked hyperkeratosis, thinned stratum malpighi, epidermal atrophy and a lichenoid dermal infiltrate
Lesions are largely asymptomatic. The overall disease course is chronic and stable with no serious complications. The primary concern of the disease is often cosmetic. Treatment is often challenging and not satisfactory, and therefore patients usually refuse aggressive therapies. With the genetic basis of the disorder now known, novel therapies enhancing sphingolipid synthesis may be on the horizon.

