Introduction
Demographics
Causes
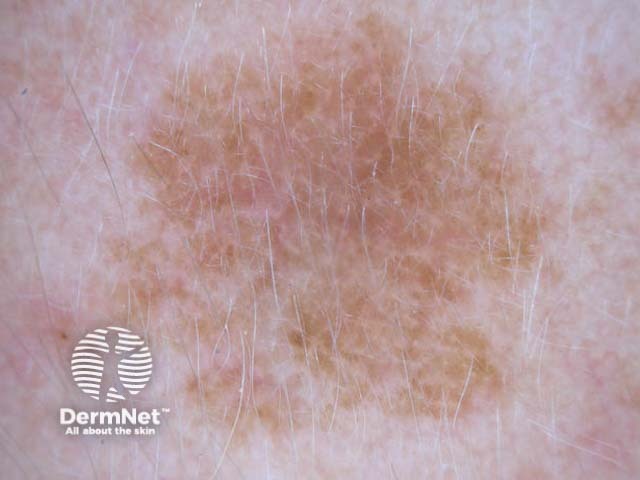
Clinical features
Variation in skin types
Complications
Diagnosis
Differential diagnoses
Prevention
Outcome
Solar lentigo is a common, benign, flat, pigmented lesion found predominantly on sun-exposed skin. It develops as a result of chronic exposure to ultraviolet radiation (UVR) from the sun or artificial sources eg, phototherapy, sunbeds.
Solar lentigines are also commonly referred to as:
Solar lentigo is associated with the following:
Solar lentigines occur due to chronic exposure to ultraviolet radiation.
While the exact pathogenesis is not fully understood, UVR is thought to cause mutations that enhance melanogenesis (melanin production) and melanin retention within keratinocytes. While melanocytic activity is increased, a key feature of solar lentigo is that the number of melanocytes within the basal cell layer is normal or only slightly increased.
Several gene mutations have been observed in both solar lentigo and seborrhoeic keratosis, suggesting a common genetic basis. These mutations include MC1R, SLC45A2, FGFR3, PIK3CA, IRF4, RALY/ASIP, and BNC2.
Solar lentigines can also occur as part of genetic syndromes such as Noonan syndrome or Peutz-Jeghers syndrome.
Solar lentigines are asymptomatic and do not cause itching or pain. Unlike ephelides (freckles), which disappear or substantially fade during winter, solar lentigo persists year-round, though it may slightly darken in summer.




Solar lentigo may be more difficult to appreciate in darker skin types.
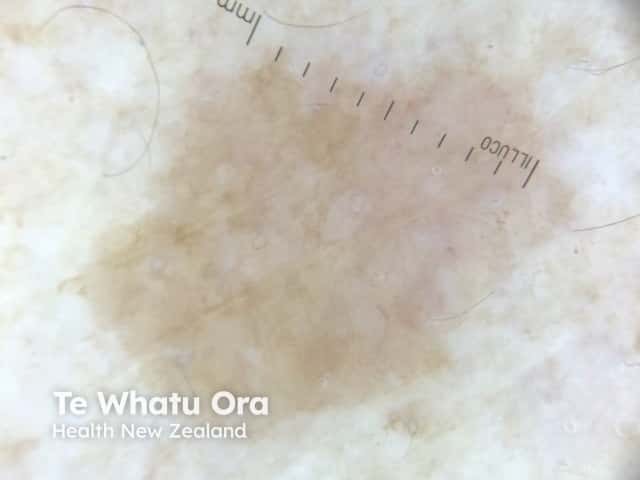
Solar lentigines are typically diagnosed clinically, aided by dermoscopy.
Dermoscopy features include:
Solar lentigines with unusual features that make it difficult to differentiate from a melanoma in situ are classified as atypical solar lentigines.
A skin biopsy should be performed where there is diagnostic uncertainty or concern for malignancy. If the lesion is variegated in colour, biopsies should be performed from each distinct area. The rationale is that different pathologies (eg, lentigo maligna, pigmented actinic keratosis) can co-exist within the same spot — these are called collision lesions.
Typical histopathological features of solar lentigo include:
See: lentigo pathology.
Solar lentigines are benign lesions that do not require treatment, unless for cosmetic reasons.
Physical
Topical
Combination-based therapy (using two or more modalities together) delivers the highest rates of resolution, followed by laser therapy, topical retinoids, cryotherapy, and peels. Destructive modalities (eg, cryotherapy, laser therapy) carry the risk of leaving behind pale or dark spots, which can be temporary or permanent.
Strict sun protection is required to prevent recurrence after treatment.
Solar lentigines can be prevented by exercising strict sun protection.
If left untreated, solar lentigines will likely persist but remain benign. Solar lentigo can slowly enlarge or darken with time, remain stable, or occasionally undergo spontaneous regression through a lichenoid reaction pattern.

