Introduction
Demographics
Causes
Clinical features
Diagnosis
Treatment
Outcome
Lichenoid keratosis is a small, inflamed macule or thin pigmented plaque, usually solitary, with a lichenoid tissue reaction on histology.



Lichenoid keratosis is also known as benign lichenoid keratosis, solitary lichen planus, lichen planus-like keratosis and involuting lichenoid plaque. It is one of the causes of atypical solar lentigo.
Lichenoid keratosis generally develops in fair-skinned patients aged 30–80 years. It is twice as common in females as than males. It is most commonly seen in Caucasians and rarely affects Asians, African Americans, or Hispanics.
Lichenoid keratosis is an inflammatory reaction arising in a regressing existing solar lentigo or seborrhoeic keratosis. It is not known what causes the reaction, but triggers can include minor trauma such as friction, drugs, dermatitis, and sun exposure.
Lichenoid keratosis may also occur in association with the PIK3CA-related overgrowth spectrum.
The clinical features of lichenoid keratosis vary depending on the inflammatory stage of the lesion.
Classic, bullous, or atypical subtype |
|
|---|---|
Clinical features |
|
Histopathology |
|
Early or interface subtype |
|
Clinical features |
|
Histopathology |
|
Late regressed or atrophic subtype |
|
Clinical features |
|
Histopathology |
|
Multiple eruptive lichenoid keratoses in sun-exposed sites are also described. Their colour varies from an initial reddish brown to a greyish purple/brown as the lesion resolves several weeks or months later.



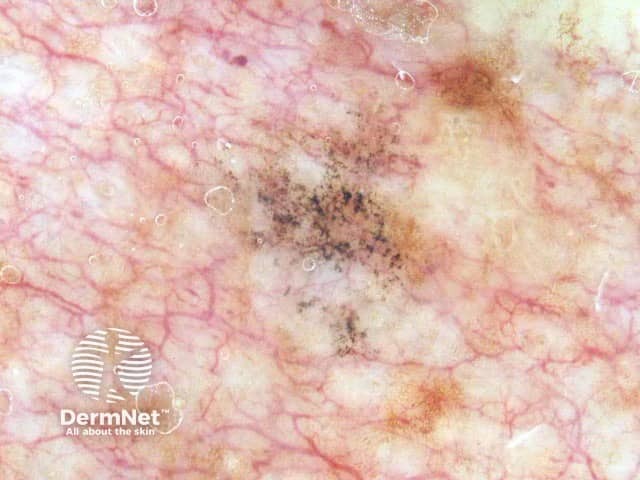
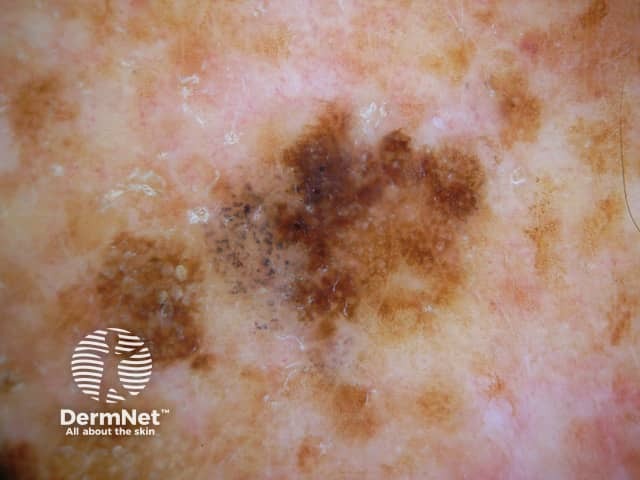
Lichenoid keratosis may be diagnosed clinically and confirmed on dermoscopy which reveals uniform clusters of grey dots [see Annular granular pattern dermoscopy]. Depending on the stage of the lesion, there may be signs of an original pre-existing lentigo or seborrhoeic keratosis which disappear with time. Later on the grey dots also disappear, as the lesion resolves.
A skin biopsy is required if clinical examination and dermoscopy cannot differentiate between lichenoid keratosis and other solitary erythematous lesions.
Histopathology resembles lichen planus or lichenoid drug eruption, with some slight differences. Remnants of the original solar lentigo or seborrhoeic keratosis may be evident.

If there is any doubt about the diagnosis, dermoscopy digital images can be taken and used in follow-up a few months later.
Lichenoid keratosis can be removed if desired by liquid nitrogen, electrosurgery or curettage.
Multiple eruptive lichenoid keratoses may be effectively treated with the oral retinoid, acitretin.
Lichenoid keratosis is harmless and resolves spontaneously.
To date there have been no reports of lichenoid keratosis turning into malignant skin tumours.

