Introduction
Demographics and causes
Clinical features
Variation in skin types
Complications
Diagnosis
Differential diagnoses
Treatment
Outcome
A syringoma is a benign adnexal tumour derived from the acrosyringium, which is the intraepidermal portion of an eccrine sweat duct. Syringomas are commonly found in clusters on and around the eyelids. They may also arise on the cheeks, scalp, axillae, umbilicus, chest, and genital regions.
Syringoma is derived from syrinx, the Greek word for tube or pipe. The Greek plural is syringomata. However, the use of ‘syringomas’ is more common.
In Friedman and Butler’s classification, four variants of syringomas are recognised:



Syringomas affect approximately 1% of the population. They are usually sporadic, appearing during or after adolescence. The male-to-female ratio is 1:2.
Familial syringomas are common, with an autosomal dominant pattern of inheritance. Inherited syringomas often arise before the onset of puberty and commonly affect the face.
Eyelid syringomas are associated with:
Eruptive syringomas are associated with:
Vulvar syringomas have an incidence of 1:1100–1500, and their appearance may be precipitated by hormonal changes, such as during pregnancy.
Clear cell syringoma is a rare variant characterised by glycogen deposition and associated with diabetes mellitus.
*Nicolau–Balus syndrome (NBS) is a rare, autosomal dominant disorder that causes a group of deformities, including: generalised eruptive syringomata, atrophoderma vermiculata, and milia cysts.
Syringomas are firm, rounded dermal papules one to three millimetres in diameter.
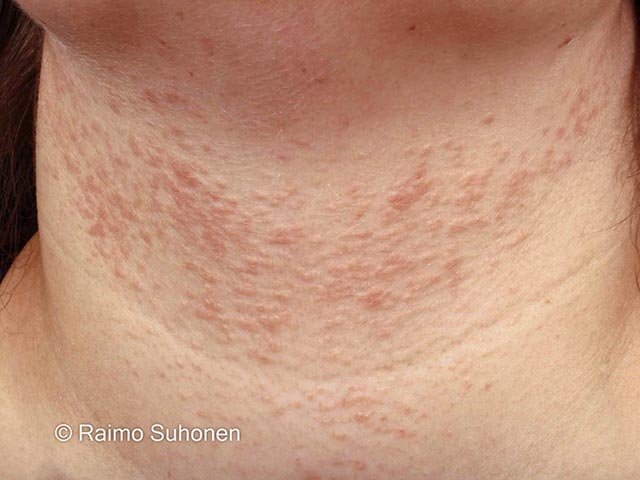
Eruptive syringomas appear as crops of hyperpigmented papules widespread across the trunk, chest, abdomen, upper extremities, female genitalia (where they are found on the labia majora) or rarely occur on the penile shaft.
Syringomas are usually asymptomatic but may cause itching associated with sweating or when located on the vulva.
In people with skin of colour, syringomas are yellowish, hypopigmented, or hyperpigmented papules.
Syringomas are benign. Their significance is primarily cosmetic.
Syringomas associated with Down syndrome may calcify (calcinosis cutis).
A syringoma is often diagnosed clinically due to its typical appearance.
A skin biopsy of syringoma reveals a normal epidermis, multiple small ducts, and epithelial cords in the dermis. Two rows of flattened epithelial cells line the ducts, the outer layer bulging outward to create a comma-like tail resembling a tadpole. The surrounding stroma is sclerotic.
Clear cell syringomas have a clear cytoplasm of the epithelial cells due to their increased levels of glycogen. When confirmed via biopsy, further evaluation for glucose intolerance is recommended due to their association with diabetes mellitus.
A full skin thickness biopsy is necessary to exclude microcystic adnexal carcinoma, which has similar features but infiltrates deep dermis and subcutaneous tissue.
The differential diagnosis for syringoma includes:
Syringomas are benign and do not require intervention. Treatment for cosmetic reasons aims to reduce tumour visibility with minimal scarring, but the results are often suboptimal.
Treatment options include:
Spontaneous regression of syringoma is rare.
Syringomas can recur after superficial treatment as they penetrate the deep dermis.
Hypertrophic or atrophic scarring and post-inflammatory pigment changes are uncommon complications of treatment, particularly in people with darker skin types.

