Capillary vascular malformations (telangiectatic naevi or nevi) are sometimes incorrectly referred to as flat haemangiomas. These are not haemangiomas but are malformed dilated blood vessels in the skin. Lesions are non-cancerous and appear as blotches of red or purple skin discolouration on any part of the body. They are always present at birth, although they may become more obvious with time. They may vary in size from a small dot to occasionally involving a whole limb, and they grow in proportion to the child's general growth.
Two common capillary vascular malformations are the naevus simplex (salmon patch) and port-wine stain (naevus flammeus).
Naevus simplex is very common and occurs in about 40% of all newborns. They are usually small flat patches of pink or red skin with poorly defined borders. They are commonly found at the nape of the neck (stork bite, erythema nuchae), on the forehead between the eyebrows (angel's kiss) or on the eyelids. They become more intense in colour and noticeable when the child is crying. Most lesions will spontaneously disappear within the first year of life. Stork bites tend to be more persistent and may remain unchanged into adult life in 50% of cases.



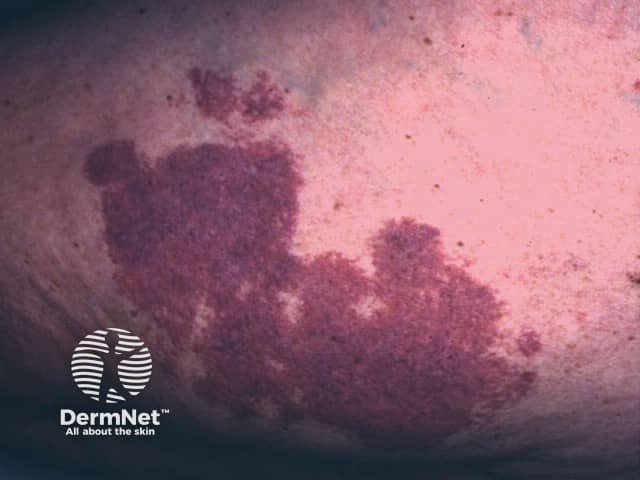
Port-wine stains are much less common than salmon patches, occurring in about 0.3% of newborns. A port-wine stain is usually a large flat patch of purple or dark red skin with well-defined borders. At birth the surface of the port-wine stain is flat, but in time it becomes bumpy and often more unsightly. The face is most commonly affected although they can occur anywhere on the body. Where present, they generally appear on one side of the body with a sharp mid-line cut-off.
Some port-wine stains may fade over time but most remain unchanged or may even deepen in colour. They do not shrink by themselves or disappear spontaneously. If the port-wine stain affects the face and neck, it may have a severe impact on the child's social, psychological and economic development.





Most capillary vascular naevi are not associated with other abnormalities. However, there are some rare syndromes that may present with this kind of birthmark:
Sturge–Weber syndrome is also known as encephalotrigeminal angiomatosis. It is the association of capillary vascular malformation affecting the skin supplied by one branch of the trigeminal nerve of the face with defects in the underlying tissues. These may result in a shrunken brain, calcification inside the skull, seizures, meningeal angioma and eye abnormalities (glaucoma, optic atrophy). Sturge-Weber syndrome is due to somatic mutation in the gene GNAQ.
Parkes-Weber syndrome refers to the association of a capillary vascular malformation with an arteriovenous malformation. The birthmark tends to be quite large. It is often faint pink, but may also be bright red in colour. The affected limb is warmer and longer than the other side, though of normal shape. It may be possible to feel a ‘thrill’ due to the high flow of blood through the arteriovenous malformation. The doctor listening with a stethoscope may hear a swishing sound or ‘bruit’. Occasionally there is enlargement of the heart, which can lead to heart failure.
Klippel-Trénaunay syndrome, part of the PIK3CA-related overgrowth spectrum, refers to the association of a capillary vascular malformation with a venous and a lymphatic malformation. The surface red birthmark tends to be small or patchy but prominent. The lymphatic malformation can contain large fluid-filled cysts (macrocystic) or clusters of smaller ones (microcystic). The affected limb is wider and bulkier than the other side, and sometimes longer. Sometimes the affected limb is smaller than the other one. The syndrome can be complicated by blood clots (thrombophlebitis), seepage of lymph, infections (cellulitis), ulceration and bleeding.
Hyperkeratotic cutaneous capillary-venous malformation usually affects the tissues around the eye. It may be associated with vascular malformations in the brain, known as ‘cavernomas’. This disorder is inherited as an autosomal dominant abnormality, affecting half the children of an affected person. It is due to a mutation in a gene called KRIT1.
Proteus syndrome is very rare and is thought to be due to an abnormal PTEN tumour-suppressor gene. It has very variable manifestations such as enlarged hands and feet or one side of the body, various birthmarks including vascular malformations, connective tissue naevi, epidermal naevi, skull abnormalities and fatty tumours (lipomas) under the skin and internally.
CLAPO syndrome is caused by sporadic mutations of the PIK3CA gene. It presents with capillary malformation of the lower lip, lymphatic malformation of the face and neck, asymmetry, and partial or generalised overgrowth.
Reticulate vascular naevi are closely related to port-wine stains. The main difference is that reticulate naevi usually spontaneously improve by fading with time.



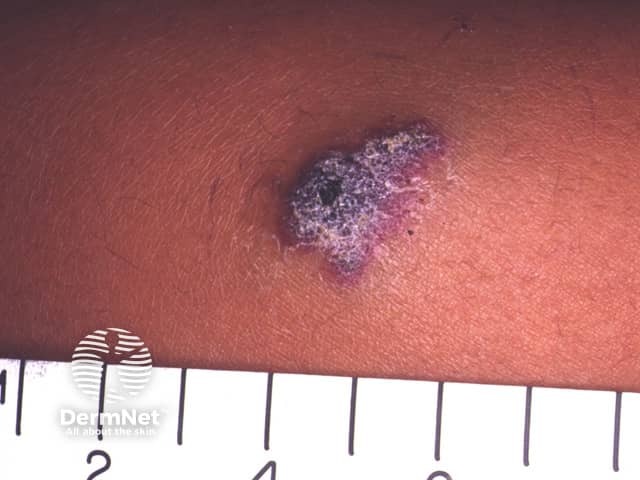
Angiokeratoma circumscriptum is a raised warty dark red-purple lesion that is most commonly found on the lower leg or foot. It is often covered with rough scaly patches of skin. In many cases, they are present at birth but may also develop in childhood or adulthood. Angiokeratomas are mostly harmless vascular lesions that usually do not require treatment.
Capillary vascular malformations are now known due to genetic abnormalities and are often familial. Investigators have found a mutation in the GNAQ gene on chromosome 9q21 in the vast majority of patients with port-wine stains and Surge-Weber syndrome.[2]
Capillary vascular malformations are usually diagnosed clinically and no investigations are necessary for the majority of flat lesions. However, when there is uncertainty about the diagnosis or whether underlying tissues are affected, an ultrasound scan is often performed. Characteristically, a vascular malformation shows blood vessels set in normal background tissue.
In more complicated cases it may be necessary to perform Magnetic Resonance Imaging (MRI) or angiography to help plan treatment.
Salmon patches require no treatment, whilst treatment of port wine stains depends on the body site, extent and nature of the lesion. In the past, a cosmetic cover was the best advice for those affected, but now many can be successfully removed or their appearance improved by laser treatment. Specialist advice and referral for treatment are best before school entry, when possible.
The pulsed dye laser (PDL) appears to be the treatment of choice for most port-wine stains. Approximately 40–45% improve by at least 75% after 5 to 25 treatments. Some lesions that do not respond to a PDL may improve when treated with other types of laser.
Capillary vascular malformations may bleed after minor trauma and sometimes the bleeding can be difficult to stop despite the application of pressure. This is uncommon.
Complex syndromes require careful assessment, often by a team of specialists that may include a paediatric dermatologist, paediatrician, radiologist, plastic surgeon and/or vascular surgeon. The following measures may rarely be necessary:
Oral sirolimus (which inhibits angiogenesis) is undergoing investigation as a potential medical treatment for severe vascular malformations but may have significant adverse effects [1].


