Introduction Demographics Causes Clinical features Variation in skin types Complications Diagnosis Differential diagnoses Treatment Outcome
Dermatitis herpetiformis (DH) is an inflammatory immunobullous disease of the skin and a cutaneous manifestation of coeliac (celiac) disease, a gluten-sensitive enteropathy.
The name herpetiformis is derived from the tendency for blisters to appear in clusters, resembling herpes simplex. However, DH is not due to viral infection.
DH is also known as Duhring-Brocq disease.






More images of dermatitis herpetiformis
DH presents as intense itch and a symmetrical blistering rash. Vesicles (often 3–5 mm in diameter) or blisters develop on erythematous skin but are often eroded and crusted due to scratching.
DH may be exacerbated by some medications (eg, potassium iodide, non-steroidal anti-inflammatory medications, leuprolide acetate, progesterone), and premenstrually.
Images of dermatitis herpetiformis
While uncommon, clinical features are similar, although postinflammatory pigmentation is more prominent.
The following conditions may affect patients with dermatitis herpetiformis (DH), especially when it is associated with coeliac disease:
*The risk of NHL is increased six to tenfold among DH patients. Strict adherence to a gluten-free diet reduces this rare but serious complication. Fortunately, increased lymphoma risk is evident only during the first 5 years after DH diagnosis and gluten-free diet adherence.
Skin biopsy is usually necessary to confirm DH.
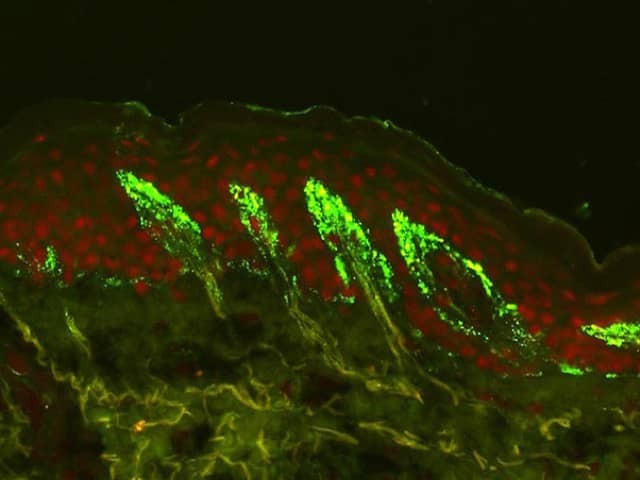
Lesional skin may show:
Uninvolved perilesional skin contains a significantly greater number of IgA deposits, and lesional biopsies in general have a higher false negative rate.
See Dermatitis herpetiformis pathology for more information.
Patients with DH are commonly offered the same blood tests used for patients with coeliac disease to screen for nutritional deficiencies. These include:
Mild anaemia may be caused by iron or folic acid deficiency (or both) due to malabsorption associated with gluten-sensitive enteropathy. Thyroid function tests are usually recommended due to the association between DH and thyroid disease.
Specific autoantibody tests for DH are:
Borderline results may be difficult to interpret.
DH patients with abnormal blood results usually proceed to have a small intestinal biopsy to confirm gluten-sensitive enteropathy. This is histologically characterised by small bowel villous atrophy. This means that instead of being highly convoluted, the lining of the intestines is smooth and flattened.
The small bowel may appear normal because of treatment (gluten-free diet and/or medication), skip lesions (the sample was taken from an unaffected site), or the intestine may be unaffected by the disease.
HLA haplotype testing (for a set of DNA variations) may reveal HLA-DQ2 or HLA-DQ8. This is present in almost all patients with DH (and coeliac disease).
A gluten-free diet for life is strongly recommended in patients with DH, as it:
It may take up to 2 years for a gluten-free diet to reach its maximal effect.
Dapsone is the treatment of choice for DH, as it usually reduces itch within 3 days.
If intolerant or allergic to dapsone, the following may be useful:
There are reports that combination therapy with dapsone and sulfasalazine may be effective in patients who do not tolerate increasing doses of dapsone monotherapy.
Topical dapsone 5% gel was also shown to be effective as an adjuvant treatment for DH. Compared to oral dapsone, topical dapsone was associated with a lower incidence of side effects and can be administered safely in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency.
Dermatitis herpetiformis usually has a good prognosis, with the majority of patients responding well to a strict gluten-free diet and medication. A lifelong gluten-free diet is required. Although the overall incidence of T cell lymphoma is increased in DH, the overall disease mortality is lower than the general population, possibly due to a reduction in cardiovascular disease and obesity.

