

Splinter haemorrhage — extra information
Introduction Demographics Causes Clinical features Complications Diagnosis Treatment Outcome
What is a splinter haemorrhage?
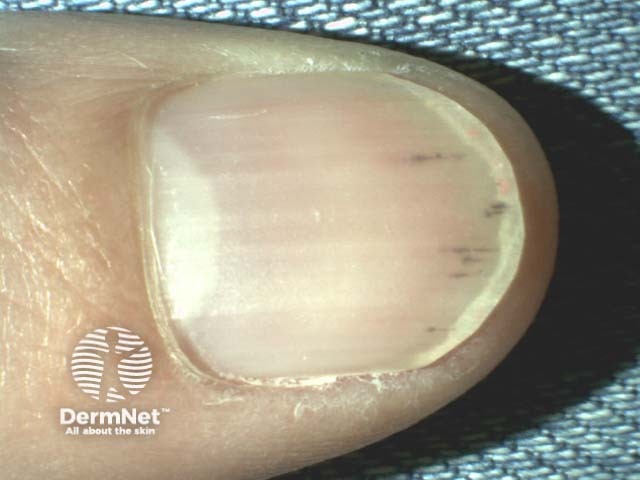
A splinter haemorrhage is a longitudinal, red-brown haemorrhage under a nail and looks like a wood splinter. Seen end-on, the haemorrhage is in the lower part of the nail plate or underneath it.


Who gets splinter haemorrhages?
Splinter haemorrhages can occur at any age; however, they are more common in older people [1,2].
- In healthy individuals, splinter haemorrhages occur more frequently in men than women.
- Splinter haemorrhages are more frequent in dark-skinned people than in light-skinned people.
- The characteristics of patients who develop splinter haemorrhages relate to their underlying cause.
What causes splinter haemorrhages?
The most common cause of a splinter haemorrhage is trauma, including the application of an acrylic nail [3]. The longitudinal nature of splinter haemorrhages is explained by the orientation of the capillaries in the nail bed.
Infection
Splinter haemorrhages are present in 15–33% of patients with infective endocarditis in association with Osler nodes and Janeway lesions [3]. They may be due to septic emboli in the small vessels of the nail bed and the increased fragility of the vessel walls in sepsis [2,3].
Other infective causes include:
- Meningococcal disease
- Psittacosis
- Disseminated histoplasmosis.
Skin disease
Splinter haemorrhages are common signs of psoriatic nail disease and nail disease due to lichen planus [3]. They can also be associated with a tumour.



Systemic diseases
Splinter haemorrhages may be due to microemboli or injury to vessel walls associated with vasculitis, including systemic diseases such as [3]:
- Primary antiphospholipid syndrome
- Systemic lupus erythematosus
- Raynaud disease
- Behcet disease
- Cutaneous vasculitis
- Scurvy.
Splinter haemorrhages are observed in patients with chronic kidney disease on haemodialysis or post-renal transplant, and may be explained by abnormal coagulation [3].
Drugs
Medications associated with splinter haemorrhages include [3]:
- Tyrosine kinase inhibitors (seen in 60–70% of patients taking sunitinib and sorafenib)
- Nitrofurantoin
- Ganciclovir
- Terbinafine
- Tetracyclines.
What are the clinical features of splinter haemorrhages?
Splinter haemorrhages present as longitudinal 1–3 mm red lines under the nail plate [2,3].
- They can be single or multiple.
- They may be asymptomatic or tender.
- The red line moves distally with time (weeks to months).
- Haemorrhages under the distal third of the nail plate are frequent and are usually a result of trauma such as a sports injury. They may be associated with subungual haematoma and nail splitting.
- Proximal haemorrhages, especially affecting multiple fingernails, are more likely due to a systemic disease, especially in women.
What are the complications of splinter haemorrhages?
There are no complications of splinter haemorrhages themselves; complications arise as a consequence of the underlying disease process.
How is a splinter haemorrhage diagnosed?
A careful history and physical examination are required to determine the underlying cause.
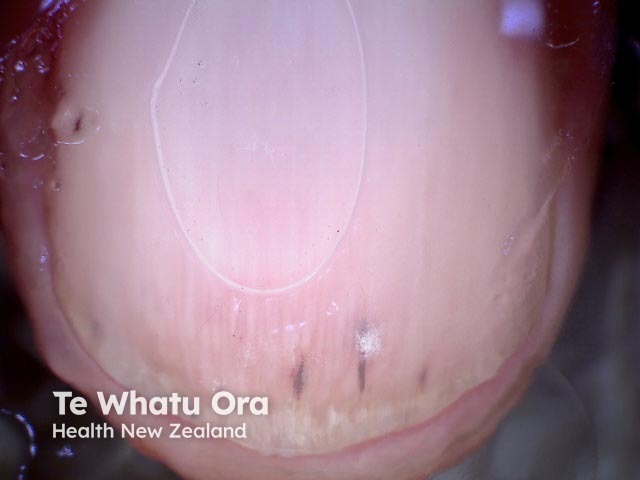
The diagnosis of splinter haemorrhages is made clinically or with the aid of dermatoscopy [1].


What is the treatment for a splinter haemorrhage?
There is no specific treatment for a splinter haemorrhage.
Any treatment is targeted at an underlying systemic condition or at discontinuing a causative drug.
What is the outcome for a splinter haemorrhage?
If caused by trauma, a splinter haemorrhage grows out and disappears. Haemorrhages may continue to recur if the underlying cause remains.
References
- Tosti A, Piraccini BM. Nail disorders. Dermatology, 71, 1203–19
- Baran R, Dawber RPR. Diseases of the nails and their management, 4th edn. Chichester: John Wiley & Sons, 2012.
- Haber R, Khoury R, Kechichian E, Tomb R. Splinter haemorrhages of the nails: a systematic review of clinical features and associated conditions. Int J Dermatol 2016; 55: 1304–10. PubMed
On DermNet
- Bleeding and bruising
- Subungual haemorrhage
- Subungual haemorrhage images
- Psoriatic nail dystrophy
- Lichen planus
- Nail disorders