

Lichen planopilaris — extra information
Introduction
Demographics
Causes
Clinical features
Variation in skin types
Complications
Diagnosis
Differential diagnoses
Treatment
Outcome
What is lichen planopilaris?
Lichen planopilaris is an uncommon inflammatory condition that can lead to permanent hair loss.
The disease is considered to be a form of lichen planus which affects the hair follicles. It results in patchy, progressive, permanent hair loss mainly on the scalp, although other hair bearing skin (brows, pubic, and body) may be affected. Several forms are recognised:
- Classic lichen planopilaris, also known as follicular lichen planus
- Frontal fibrosing alopecia
- Graham Little syndrome.




Who gets lichen planopilaris?
- Lichen planopilaris usually affects young adult women, although the age range is wide and it can also affect men.
- It commonly develops in association with lichen planus affecting the skin, mucosae, and nails.
- Although lichen planopilaris is rare, it is one of the common causes of scarring hair loss of the scalp.
What causes lichen planopilaris?
The exact cause of lichen planopilaris is unknown. It is thought to be a cytotoxic autoimmune response to an unknown antigen located in hair follicles. The disease is rarely gene-related. It is also rarely drug-induced, eg, pembrolizumab.
What are the clinical features of lichen planopilaris?
Lichen planopilaris typically presents as smooth white patches of scalp hair loss. No hair follicle openings can be seen in the areas of hair loss. Scale and redness surround each hair follicle at the edges of these patches, which may be spiny on palpation. Hairs can be easily pulled out. It is multifocal and small areas may merge to form larger irregular areas.
Common sites of involvement are the sides, front, and lower back of the scalp.
Symptoms are often absent, but they may include:
- Itch
- Pain
- Tenderness
- Discomfort
- Burning.
Lichen planopilaris is usually slowly progressive.
Diffuse hair loss is uncommon.
How do clinical features vary in differing types of skin?
The clinical features do not vary in differing skin types.
What are the complications of lichen planopilaris?
- Hair loss (alopecia)
- Rarely eyelash and eyebrow loss
- Psychological distress and reduced quality of life.
How is lichen planopilaris diagnosed?
Lichen planopilaris is suspected on the clinical presentation and careful examination of the mouth, nails, and skin for evidence of lichen planus elsewhere.
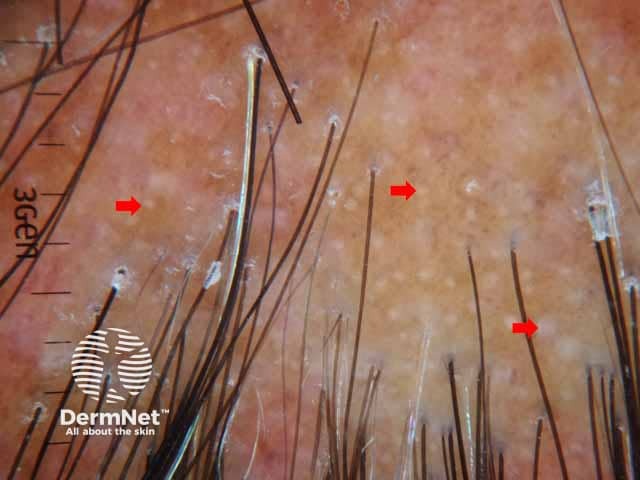
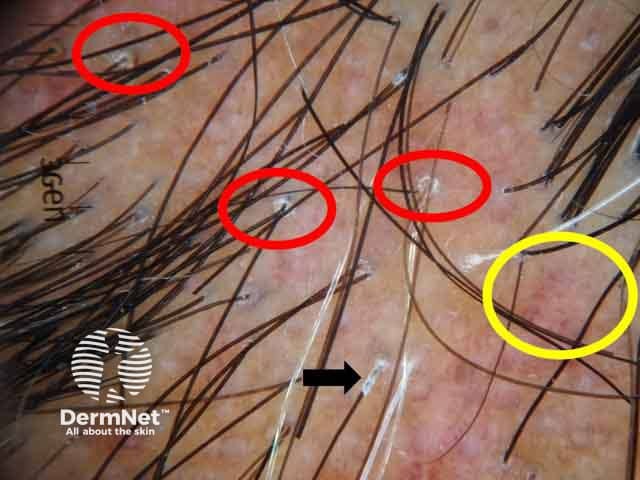
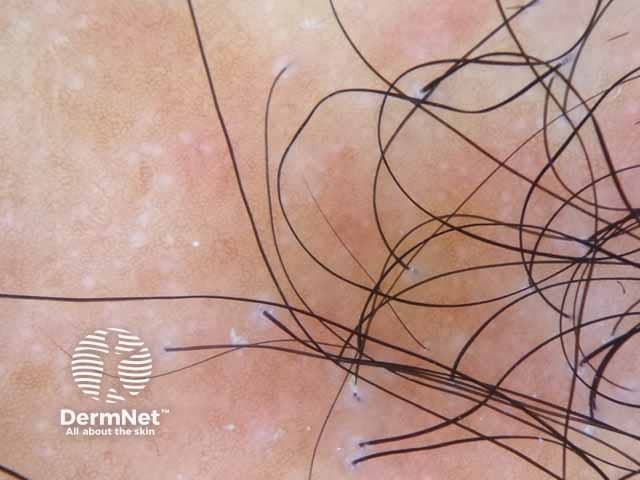
Trichoscopy reveals absent follicles, white dots, tubular perifollicular scale, and perifollicular erythema.
The diagnosis may be confirmed on scalp biopsy that includes hairs with surrounding redness and scale at the edge of an area of hair loss. Lichen planopilaris is an example of a primary lymphocytic folliculitis.
However, it is not always possible to make a diagnosis on biopsy. Where there is only patchy scarring, hair loss, and no evidence of inflammation, the diagnosis may not be able to be confirmed.
What is the differential diagnosis for lichen planopilaris?
- Discoid lupus erythematosus (DLE)
- Central centrifugal cicatricial alopecia (CCCA)
- Folliculitis decalvans
- Alopecia areata
- Pseudopelade of Brocq
What is the treatment for lichen planopilaris?
Treatment should be sought and provided early, as no treatment restores hairs that have already been lost and replaced by scarring. The aim of treatment is to slow the progression of the disease and relieve symptoms. Hair loss may continue, although at a slower rate.
Anti-inflammatory treatment options include:
- Corticosteroids — potent topical, intralesional, oral
- Topical tacrolimus
- Topical minoxidil
- Topical ruxolitinib
- Hydroxychloroquine
- Tetracycline e.g. doxycycline
- Acitretin
- Methotrexate
- Ciclosporin
- Mycophenolate mofetil
- Pioglitazone (an oral PPAR-γ agonist): variable efficacy; up to 50–70% of patients have reduced symptoms, inflammation, and disease progression
- Platelet rich plasma
- Adalimumab, a tumour necrosis factor-alpha (TNFα) inhibitor, has also been reported to be effective in a few patients
- Oral JAK inhibition with tofacitinib.
Response to treatment is variable and some published studies contradict others as to their efficacy. The best patients can expect is to stop the progression of hair loss and to minimise scalp discomfort.
A management protocol as suggested by Svigos et al. (2021) includes:
- Making a diagnosis of lichen planopilaris clinically, trichoscopically, and with a scalp biopsy.
- The severity of symptoms, the extent of hair loss, and presence of disease activity are documented at each visit, approximately every 3 months.
- Use potent or superpotent topical steroids, with topical minoxidil 5% and 0.3% tacrolimus.
- Oral hydroxychloroquine (usually 200 mg twice daily) is started after appropriate laboratory tests and eye checks if the patient is symptomatic, has progressive hair loss, or signs of active disease.
- Consider doxycycline orally if there is progression on hydroxychloroquine.
- With further progression consider immunomodulation with methotrexate or ciclosporin.
Non-pharmacological measures
- Camouflage with careful hair styling, hair colouring, and hairpieces such as wigs may be discussed with the patient.
- Surgery such as scalp reduction and hair transplantation has been used for end-stage inactive disease with large areas of scarring but is not always successful. Risks of the Koebner phenomenon and reduced graft survival are experienced.
What is the outcome for lichen planopilaris?
The prognosis of the disease cannot be predicted. It may improve on its own after a period of time, or can get progressively worse. The main goal of treatment is to stop the hair loss, but the response to treatment also varies amongst patients.
Bibliography
- Alam MS, LaBell B. Treatment of lichen planopilaris with adalimumab in a patient with hidradenitis suppurativa and rheumatoid arthritis. JAAD Case Reports 2020; 6(3): 219–21. Journal
- Babahosseini H, Tavakolpour S, Mahmoudi H, et al. Lichen planopilaris: retrospective study on the characteristics and treatment of 291 patients. J Dermatolog Treat. 2019;30(6):598–604. Journal
- Nic Dhonncha E, Foley CC, Markham T. The role of hydroxychloroquine in the treatment of lichen planopilaris: A retrospective case series and review. Dermatol Ther. 2017;30(3):10.1111. Journal
- Cho BK, Sah D, Chwalek J, Roseborough I, Ochoa B, Chiang C, Price VH. Efficacy and safety of mycophenolate mofetil for lichen planopilaris. J Am Acad Dermatol 2010; 62: 393–7. PubMed
- Mirmirani P, Karnik P. Lichen planopilaris treated with a peroxisome proliferator— activated receptor γ agonist. Arch Dermatol 2009; 145: 1363–6. PubMed
- Singal A, Ong MM, Lipner SR. Gonadocorticoid exposure is associated with increased odds of lichen planopilaris and frontal fibrosing alopecia: A large retrospective cohort study. J Am Acad Dermatol. 2025;92(2):352-354. doi:10.1016/j.jaad.2024.10.030. Pubmed
- Svigos K, Yin L, Fried L, Lo Sicco K, Shapiro J. A Practical Approach to the Diagnosis and Management of Classic Lichen Planopilaris. Am J Clin Dermatol. 2021;22(5):681–92. doi:10.1007/s40257-021-00630-7. PubMed
- Mesinkovska NA, Tellez A, Dawes D, Piliang M, Bergfeld W. The use of oral pioglitazone in the treatment of lichen planopilaris. J Am Acad Dermatol 2015; 72:355–6. Journal
- Spring P, et al. Lichen planopilaris treated by the peroxisome proliferator activated receptor-γ agonist pioglitazone: Lack of lasting improvement or cure in the majority of patients. J Am Acad Dermatol. 2013; 69;830–2. PubMed
- Williams, K. N., Perez, S. M., Burroway, B., & Tosti, A. (2025). Topical ruxolitinib in the management of frontal fibrosing alopecia and/or lichen planopilaris: A single-center retrospective cohort study. Journal of the American Academy of Dermatology, 92(1), 170–172. doi:10.1016/j.jaad.2024.09.032. Journal
- Yang CC, Khanna T, Sallee B, Christiano AM, Bordone LA. Tofacitinib for the treatment of lichen planopilaris: A case series. Dermatol Ther. 2018;31(6):e12656. PubMed Central
On DermNet
- Graham Little syndrome
- Frontal fibrosing alopecia
- Lichen planus
- Hair loss
- Pseudopelade of Brocq
- Lichenoid disorders
- Psychological effects of hair loss
Other websites
- Lichen planopilaris — British Association of Dermatologists patient information