Introduction
Demographics
Causes
Clinical features
Diagnosis
Differential diagnoses
Treatment
Outlook
Frontal fibrosing alopecia is a patterned form of scarring hair loss along the frontal scalp hair margin. It was first described in a group of Australian women in 1994.
Although the typical patient with frontal fibrosing alopecia was described as a Caucasian post-menopausal woman over the age of 50, younger women, men, and children, and all ethnic groups including Asians, Hispanics, and those of African descent can be affected.
The incidence is reported to be increasing worldwide.
Frontal fibrosing alopecia is frequently reported in patients with hypothyroidism, contact allergy to fragrances, regular sunscreen use, and autoimmune diseases including lupus erythematosus and rheumatoid arthritis.
Genetic, hormonal, autoimmune, inflammatory, and environmental factors have postulatedno roles in the pathogenesis of frontal fibrosing alopecia. Pairs of monozygotic twins with frontal fibrosing alopecia and positive family histories reported in some cases suggest a genetic tendency. An androgen-dependent aetiology has been suggested by the predominance of post-menopausal patients.
Contact allergy or photocontact allergy to cosmetics, moisturising creams, hair dye, and sunscreen have been suggested as possible but unconfirmed causative factors.
Frontal fibrosing alopecia has been considered a variant of lichen planopilaris due to the resemblance on histology and an association with various forms of lichen planus, but there are also many differences that raise doubts.
Frontal fibrosing alopecia usually presents as a uniform linear band of hair loss along the front and sides of the scalp hair margin, resulting in a receding frontal hair line. Atypical patterns of loss include a diffuse zig-zag pattern, a pseudo-fringe-sign, or continuous involvement all the way around the hair margin both front and back.
The skin in the affected area lacks the sundamage seen on the forehead, allowing assessment of the extent of the recession. It looks pale, shiny, or mildly scarred, without visible hair follicle openings. During the active phase redness and scale is visible around involved hairs. Single 'lonely' hairs often persist in the bald areas. The hair pull test is negative.
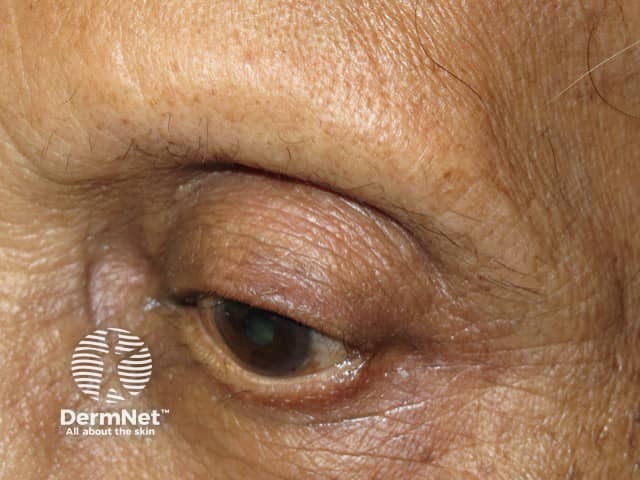
Hair loss in frontal fibrosing alopecia is usually not restricted to the frontal hairline. Eyebrow thinning or loss (madarosis) often precedes the scalp changes. Hair loss can affect all parts of the body, and almost total loss from limbs is common. In men, loss of beard and sideburns is described and may be the only site of involvement.
Itch and pain are common early symptoms, and may occur before any obvious loss of hair density. Facial rashes are another potentially early sign. These may present as skin coloured or yellowish follicular papules located on the forehead and temples, diffuse erythema or red dots around hairs.
Androgenetic alopecia (male pattern hair loss, female pattern hair loss) is commonly associated and may lead to missed diagnosis.





Dermoscopy reveals absent follicles, white dots, tubular perifollicular scale, and perifollicular erythema. In skin that tans easily, perifollicular pigmentation may be observed.
Women of African descent with frontal fibrosing alopecia present differently from Caucasian women. Typically they present at a younger age, often in their early 40s before menopause. Itch, redness, and scale are less obvious. Lichen planus pigmentosus is commonly associated, and usually precedes the hair loss. Speckled pigmentation of hair follicles along the frontal hair margin is seen on dermoscopy. Frontal fibrosing alopecia may be overlooked due to associated traction alopecia.
The clinical features of frontal fibrosing alopecia are characteristic.
Skin biopsy may be required to exclude other forms of scarring alopecia. The histopathological features of frontal fibrosing alopecia are identical to those of lichen planopilaris.
Biopsy of skin papules may also show a lichenoid pattern of inflammation, fibrosing alopecia, and sebaceous gland hyperplasia.
Diagnostic criteria have been proposed.
Major criteria:
Minor criteria:
Diagnosis requires two major criteria or one major and two minor criteria.
Recommended blood tests include haematology, biochemistry, thyroid function tests and ANA. Hormone status may assessed if there are other clinical features to suggest hyperandrogenism. Patch testing should be considered.
Androgenetic alopecia and traction alopecia often co-exist.
Other types of scarring hair loss need to be considered, but rarely share the band-like pattern of frontal fibrosing alopecia.
There is no uniformly effective treatment for frontal fibrosing alopecia to date. A short course of oral steroids, intralesional steroid injections, anti-inflammatory antibiotics such as tetracyclines, or antimalarial tablets may benefit patients who have a rapid onset of hair loss. The 5-alpha-reductase inhibitors finasteride and dutasteride have been reported to stop further hair loss but this may be due to associated androgenetic alopecia. Immunosuppressants tried include ciclosporin and mycophenolate mofetil. There has been interest in the use of low-dose oral minoxidil and low-dose naltrexone.
The use of the antidiabetic agent pioglitazone (off-label) for the treatment of frontal fibrosing alopecia was reported to reduce symptoms, inflammation, and progression of frontal fibrosing alopecia but its use has not been supported by further investigations. Side effects include ankle swelling and weight gain.
Rituximab and adalimumab are novel treatments. Topical and oral JAK inhibitors are also receiving interest as alternatives to the above immunosuppressives.
Hair grafting may be considered once disease activity has settled.
Usually, frontal fibrosing alopecia is slowly progressive although it seems to be self-limiting in most cases after several years. The hair line recedes on average of 1.8-2.6 cm. As it is a scarring alopecia, hair does not regrow unless treatment is instituted early in the process.

